Playlist
Show Playlist
Hide Playlist
Hypertension: Therapeutics


-
Slides Hypertension.pdf
-
process of diagnosis - hypercortisolism.pdf
-
Download Lecture Overview
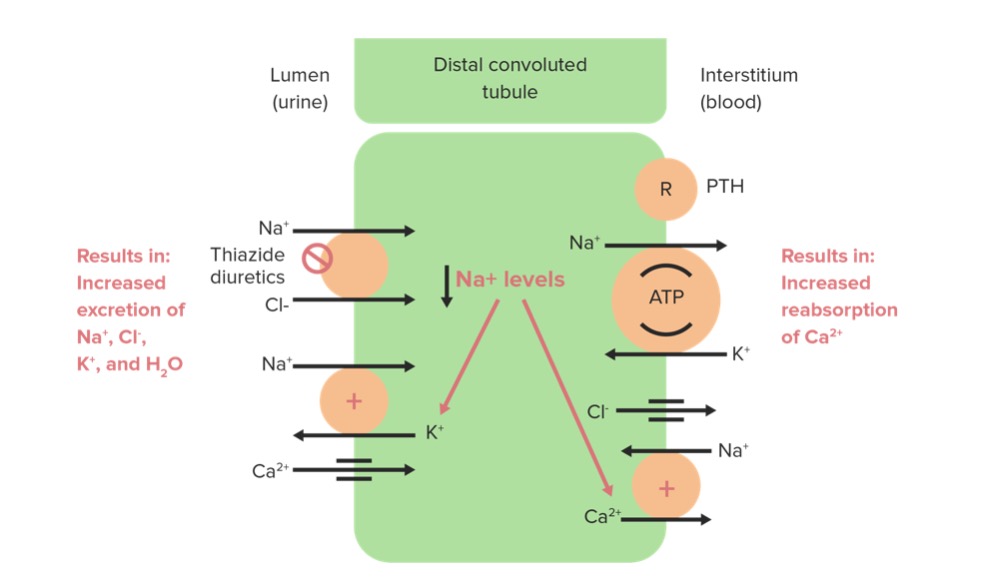
00:01 Now with this table, we are going to quickly run through this pharmaceutical agents that are then appropriate to treat different parts or different types of blood pressure. Thiazides, we've talked about this already. First line usage, patients with gout, pregnancy, electrolyte disorders, avoidance be careful, please. Because with thiazides, the fact that everyone is not able to actually retain certain things. 00:23 And thiazide tell me about its effect on calcium. It doesn't get rid of it, actually holds on to it. Where does it work? I told you earlier, works on the DCT. Works in the receptor that PTH works upon and there is every possibility that thiazide might actually reabsorb the calcium. 00:39 Keep that in mind. Beta-blockers, prior MI, stable angina, atrial arrhythmia. What are you trying to do in those patients? Well hypertension, but then if it is stable angina, remember what are you trying to do with this patient? It is the fact that you are trying to decrease the demand for oxygen by the heart instead therefore by giving beta-blockers in stable angina. Who is your patient? "Hey doc, walk a couple of blocks and I have chest pain. 01:05 I stop and the pain then goes away." Exertional angina stable. What might you want to do? Beta-blocker, hypertension. These are issues. But avoidance. If your patient already has heart block, if it is some type of let's say AV nodal type of blocks, why do you want to use that a beta-blocker? There is every possibility that you might stop the heart permanently. 01:25 Why would you want to do that? Sick sinus syndrome. Same concept here as well. It is the fact that you have arrhythmia in which there is going to be a little bit of a gap, as far as your EKG is concerned and you do not want to stop the heart permanently. COPD, remember please. If you stimulate your beta-2 receptors, albuterol, inhalers, what are they going to do? Bronchodilate. So please make sure that you pay attention to in great detail as to when you use the beta-blocker to make sure that your patient is not suffering from bronchospasms because then you may exacerbate it. Same thing with asthma. Let us continue. 02:01 ACE inhibitor. You tell me automatically, if your patient has diabetes mellitus, ACE inhibitors would be a good thing. ACE inhibitors would be contraindicated in which patient please? Talked about this a number of times. Atherosclerosis. Remember the patient, in the body requires angiotensin II to then preferentially work on which arterial? Efferent. You constrict it. You are going to restore GFR. And so therefore by giving ACE inhibitor, all you are going to do is exacerbate. So make sure that you pay attention. Pregnancy, renal vascular hypertension and angioedema are conditions in which you try to avoid ACE inhibitors at all cost. Duffy pregnancy because it is the teratogen, not only is going to work on the pregnant lady, but it is going to kill that fetus. You kill the fetal kidneys and you don't want that. ARBs, heart failure, diabetes, kidney disease pretty much the same as you hear as well. Calcium channel blockers, atrial arrhythmia and especially Raynaud syndrome. When is your patient Raynaud? They walk out into the cold. When they walk out in the cold, what make then happen to the fingers? You may then have aggregation. 03:07 You might actually have cryoglobulinemia. And when you do so, then what then happens to the digits? The digits then may become bluish and cyanotic. Welcome to Raynauds. And so, therefore, you are thinking about using calcium channel blocker. However, avoidance once again, heart block, sick sinus, pregnancy and heart failure. Aldosterone receptor blockers and you have once again prior MI, heart failure. Pregnancy and hyperkalemia, definitely avoid by giving, remember, don't forget this. Aldosterone normally exists to get rid of your potassium. If your patient already has hyperkalemia, may be secondary to renal failure, and you give an aldosterone blocker, the effects of aldosterone had been lost. What are you going to do? You are going to exacerbate the hyperkalemia. And what is that going to affect? It is going to affect your heart. Isn't that the number one organ that you worried about? Absolutely and so, therefore, you might have T tenting as you should know.
About the Lecture
The lecture Hypertension: Therapeutics by Carlo Raj, MD is from the course Hypertension: Basic Principles with Carlo Raj.
Included Quiz Questions
Which of the following is a first-line drug in the management of hypertension?
- Triamterene-hydrochlorothiazide
- Doxazosin
- Aspirin
- Clonidine
- Furosemide
Which of the following drugs is contraindicated in patients with reactive airway disease?
- Propranolol (non-selective beta-blocker)
- Verapamil (calcium channel blocker)
- Enalapril (ACE inhibitor)
- Spironolactone (diuretic)
- Losartan (angiotensin receptor blocker)
Which class of anti-hypertensive medications is contraindicated in patients with hyperkalemia?
- Aldosterone receptor blockers
- Calcium channel blockers
- Beta blockers
- Antimuscarinics
- Alpha blockers
Author of lecture Hypertension: Therapeutics

Carlo Raj, MD
Customer reviews
4,6 of 5 stars
| 5 Stars |
|
4 |
| 4 Stars |
|
0 |
| 3 Stars |
|
1 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Muy buena clase, muy dinámico y claro a la hora de explicar, 100% recomendada, además enfatiza en temas importantes
Great explanation, simple but effective. I just watch videos in hypertension in cardiology playlist. When the quiz pop up, I answer them all ????% correctly. What does that mean? The explanation in the video is easy to remember. Really, if I have money, I wanna subscribe for 1 year and watch all the video. Thank you for the great lecture, Lecturio. From Indonesia
love it i was able to remember the videos kept my attention
Good for refreshing ,anybody can review it once because , it quick and easy explanation .
