Playlist
Show Playlist
Hide Playlist
Tachycardia: Multifocal Atrial Tachycardia: Pathogenesis


-
Slides Tachyarrhythmia MultifocalAtrialTachycardia CardiovascularPathology.pdf
-
Download Lecture Overview
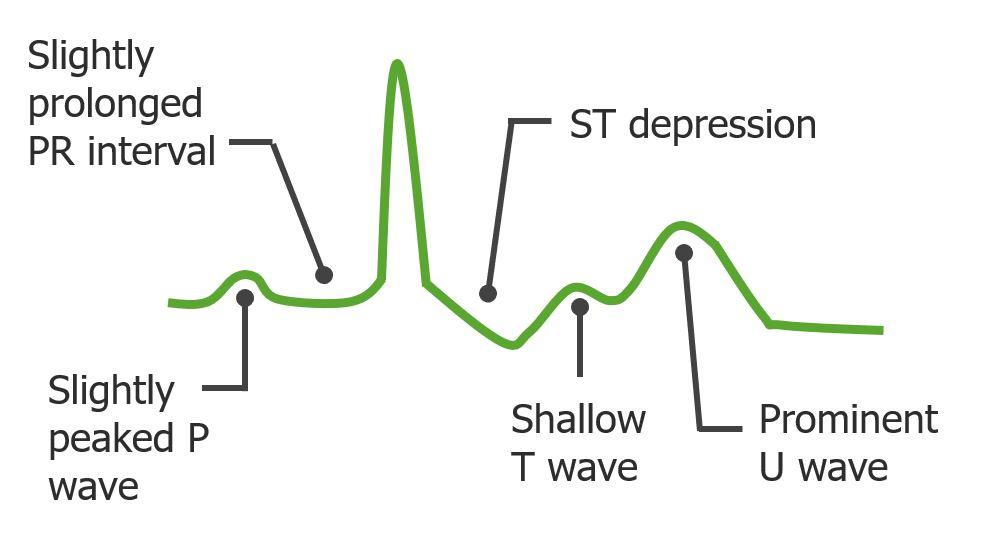
00:01 Let us continue. We will take a look at supraventricular tachycardias. The way that this is set up is so that we haven't given you all four. I haven't given you all four. Tachyarrhythmia is here so that you are not confused as to which one is which. There was a discussion with atrial flutter and atrial fibrillation and we distinguished between the two very clearly, primarily in terms of its description, irregularly irregular would be which one? Atrial fibrillation. If it is regular and you have a 2:1 type of pattern, which means two P waves for every one QRS complex, then you have a regular rhythm and this will then bring us to flutter and saw-tooth. So these were the two supraventricular tachycardias that you need to make sure that you know in great detail and then here we will take a look at two others. One known as multifocal atrial tachycardia. Now we will do the same thing. Do not allow the name to fool you, confuse you and frustrate you, in fact, used the name to then clue you when as to the diagnosis of your patient. So multifocal atrial tachycardia is once again dealing with the atria, thus, it is a SVT, a supraventricular tachycardia. 01:18 Keep in mind that the objective at all times is to make sure that you prevent these tachycardias from entering the ventricles. Due to focal pacemaker abnormalities, I will tell you what that means in a second and what end up happening here is a multifocal or multiple ectopic pacemaker firing. And by a pacemaker, we are referring to our SA node. Thus, the P wave is going to be quite operative for us to pay attention to, leading to tachycardia of course. Rapid abnormal P wave, well that once again doesn't tell you a whole lot except for the fact that this is an SVT, right. And once again obviously here, this is before the QRS complex. That is so much obvious, but the abnormality in the P wave is taking place prior too. 02:09 The patients well, here once again because you have tachy. Well, the heart is feeling a little pulsating thus palpations. You have irregular heart rate, fatigue, and angina, dyspnea well rest of these are pretty nonspecific, you would find these with pretty much any SVT. Here once again the causes overlap with a lot of SVTs including hypertension. We saw this that atrial fibrillation, hypertension. 02:41 How do the patients could be a possible etiology moving into atrial fibrillation. So how do we know? Atrial fibrillation. What happen to those P waves? They were fibrillated. In other words, they were obscured, difficult to find, wavy pattern, not saw-tooth, irregularly irregular. So when we get closer to the EKG that you are responsible for identifying, you will take a look at the pattern of P wave that we will see here with MAT, multifocal atrial. IHD, ischemic heart disease; hypothyroidism, alcohol, pulmonary embolism, well all of these once again would result in multiple types of SVTs and it really is up to you to make sure that you take each one of these SVTs that we are looking at commonly as by basically any professional including licensing exam. And how do you distinguish amongst the SVTs is what we are doing, aren't we?
About the Lecture
The lecture Tachycardia: Multifocal Atrial Tachycardia: Pathogenesis by Carlo Raj, MD is from the course Arrhythmias: Basic Principles with Carlo Raj.
Included Quiz Questions
Which of the following statements is correct regarding multifocal atrial tachycardia?
- ECG shows rapid abnormal P waves.
- ECG shows an absence of P waves.
- Hypothyroidism can cause multifocal atrial tachycardia.
- ECG shows a sawtooth appearance of P waves.
- The rhythm is regular.
What is not a common cause of multifocal atrial tachycardia?
- Hypothyroidism
- Hypertensive heart disease
- Ischemic heart disease
- Alcohol ingestion
- Pulmonary embolus
Author of lecture Tachycardia: Multifocal Atrial Tachycardia: Pathogenesis

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
