Playlist
Show Playlist
Hide Playlist
Tachycardia: Atrial Fibrillation: Treatment


-
Slides Tachyarrhythmia Atrial Fibrilation Cardiovascular Pathology.pdf
-
Download Lecture Overview
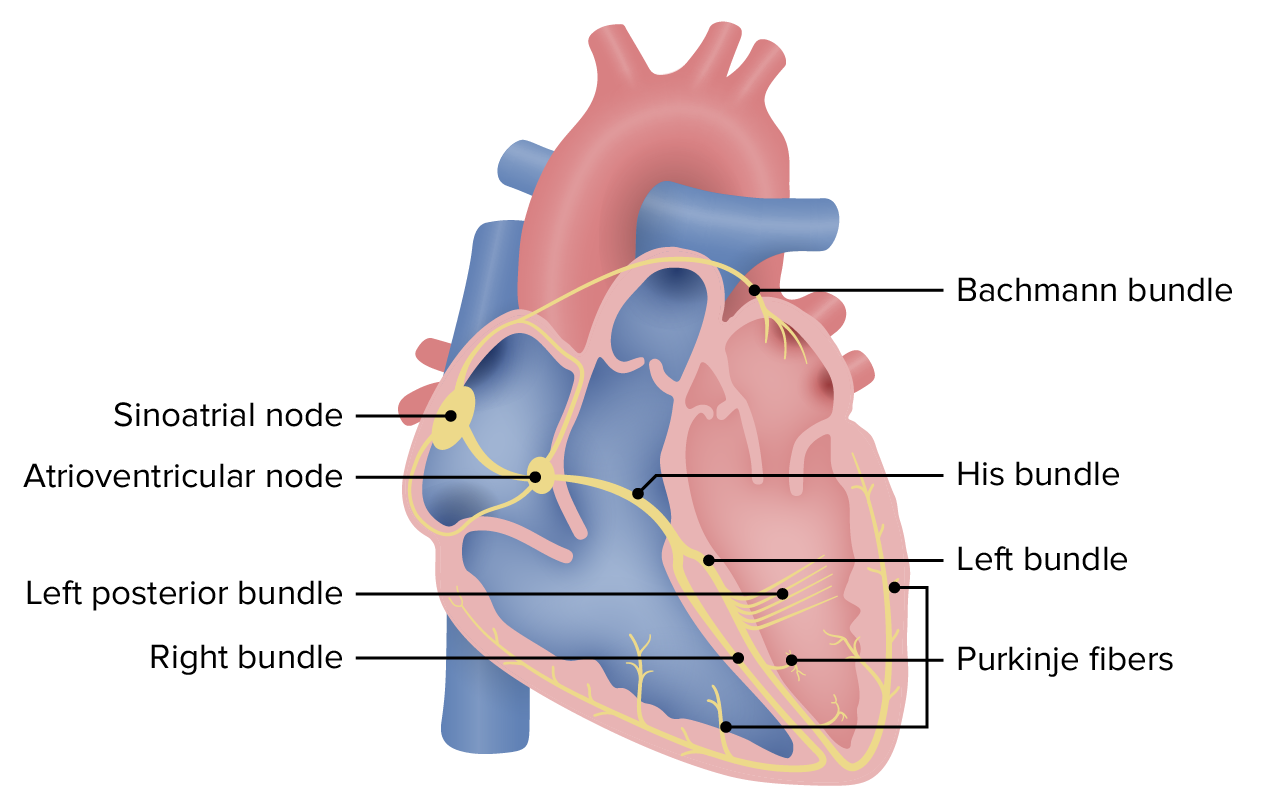
00:00 Atrial fibrillation, you want to control that rate. You want to control that rhythm and decreased risk of embolic stroke. That is your objective for management. Is that clear? When you do these, then for the most part, you should be able to manage your patient effectively. How do you control the rate? Ray Control and a patient with atrial fibrillation can be achieved by slowing AB neuro conduction. 00:24 This can be done with non dehydrating calcium channel blockers such as dull, tiresome, or beta blockers such as metoprolol. 00:31 Esmail or propranolol given I.V. 00:34 for chronic management. 00:35 Oral agents include dull, tiresome, verapamil atenolol and metoprolol as well as others. 00:42 Historically, digoxin was used more often and amiodarone may be used in more severe cases. 00:47 Rhythm control. How do you do this? You re-establish your sinus rhythm. What does sinus mean to you? Sinoatrial and that sinus rhythm was completely irregular. Anti-arrhythmic medication such as? Well it depends, right. It really depends. Now at this point what I would like for you to do from pathology? Because at some point when you bring in the management issues or the management administration, you want to understand the concept first and then maybe chose a drug that makes more sense for that particular arrhythmia, okay. So at this point, while you are thinking about the SA node, you are thinking about things like the action potential 403 with SA node. What are they? 4, 0, 3. So what is the deep polarization phase here for an SA node? Phase 0. Is that sodium channel? Not for an SA node. It is the calcium channel. Is that clear? Phase IV you control by giving a beta-blocker. A class II type anti-arrhythmic. 01:56 All I am doing here is lying down the foundation or should I say reinforcing the foundation. 02:02 So then we understand the pathology and how you manage this. If at this point, if you are confused, if you are a little frustrated or if you have lost what I have just said, repeat what I am telling you and take a look at your normal physiology of two action potentials in the heart and then take a look at anti-arrhythmic drugs and you put all this together, alright. 02:25 Then you do electrical cardioversion. At some point, you have to cardiovert. You have to. 02:30 Because when you talk about atrial fibrillation, because you want to get that rhythm under control. 02:36 Decreased risk of embolic stroke. Now this one we have mentioned a few times. You want to use anticoagulation. You are worried about CVA, which stands for cerebrovascular accident, a.k.a. stroke and you could prevent this from happening by giving a warfarin. In other words, Stroke risk can be decreased with aspirin, warfarin or direct acting oral anticoagulants such as apixaban and rivaroxaban. 02:58 It is helpful to calculate whether a patient with atrial fibrillation is low risk or high risk, which can be done using a tool called the Chads two vasc for which we will show on the next slide. 03:08 Patients with a chance to VASC score of zero or one are considered lower risk and can be managed with aspirin alone. 03:14 Patients with a score of two or higher should be managed with anticoagulation unless contraindicated These include warfarin or direct oral anticoagulants. 03:23 Warfarin is used in patients with valvular heart disease or with mechanical heart valves and requires frequent monitoring of the lab test, pro time or INR to make sure they are therapeutically anticoagulated. 03:34 Patients with nonvalvular atrial fibrillation can be managed with direct oral anticoagulants, such as a factor ten inhibitor listed on the slide or direct thrombin inhibitor typically outran no lab monitoring of the INR as needed with these medications. 03:48 The chance to VASC score helps determine the risk of stroke in an individual with atrial fibrillation in the old system, simply called chads, the C stood for CHF history aged for hypertension, A for age, the D for diabetes and the S for previous stroke or TIA symptoms. 04:05 This was replaced in 2012 with the chads two VASC scoring for anticoagulation determination in patients with A-fib. 04:12 Basically, you score one point each for history of CHF hypertension age 65 to 74 diabetes, female sex and history of vascular disease, which includes prior myocardial infarction, peripheral artery disease or aortic plaque. 04:29 You give two points if the patient is age 75 or older and two points if they have a past history of stroke or TIA. 04:35 So in total if a patient scores two or more there's a clear benefit of anticoagulation in preventing stroke.
About the Lecture
The lecture Tachycardia: Atrial Fibrillation: Treatment by Carlo Raj, MD is from the course Arrhythmias: Basic Principles with Carlo Raj.
Included Quiz Questions
Which of the following is NOT a major goal in managing atrial fibrillation?
- Improve inotropic effect
- Rate control
- Prevent thromboembolism
- Prevent stroke
- Rhythm control
Which of the following is NOT a drug commonly used in the management of atrial fibrillation?
- Lidocaine (Class Ib antiarrhythmic)
- Warfarin
- Digoxin
- Beta blockers
- Apixaban (factor Xa inhibitor)
A 58-year-old man with a medical history significant for hypertension and diabetes mellitus presents with atrial fibrillation. He has no history of congestive heart failure, previous stroke, or TIA. What is his CHA2DS2-Vasc score risk for stroke and how would you manage him?
- Score = 2; treat with warfarin
- Score = 3; treat with aspirin
- Score = 1; no anticoagulation needed
- Score = 2; treat with aspirin
- Score = 4; treat with warfarin
Author of lecture Tachycardia: Atrial Fibrillation: Treatment

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Muy completa la explicación y clara, además de correlacionar muy bien la fisiología con la clínica y semiología. Muy buenos tips semiológicos.
