Playlist
Show Playlist
Hide Playlist
Syncope: Evaluation, Treatment, and Management

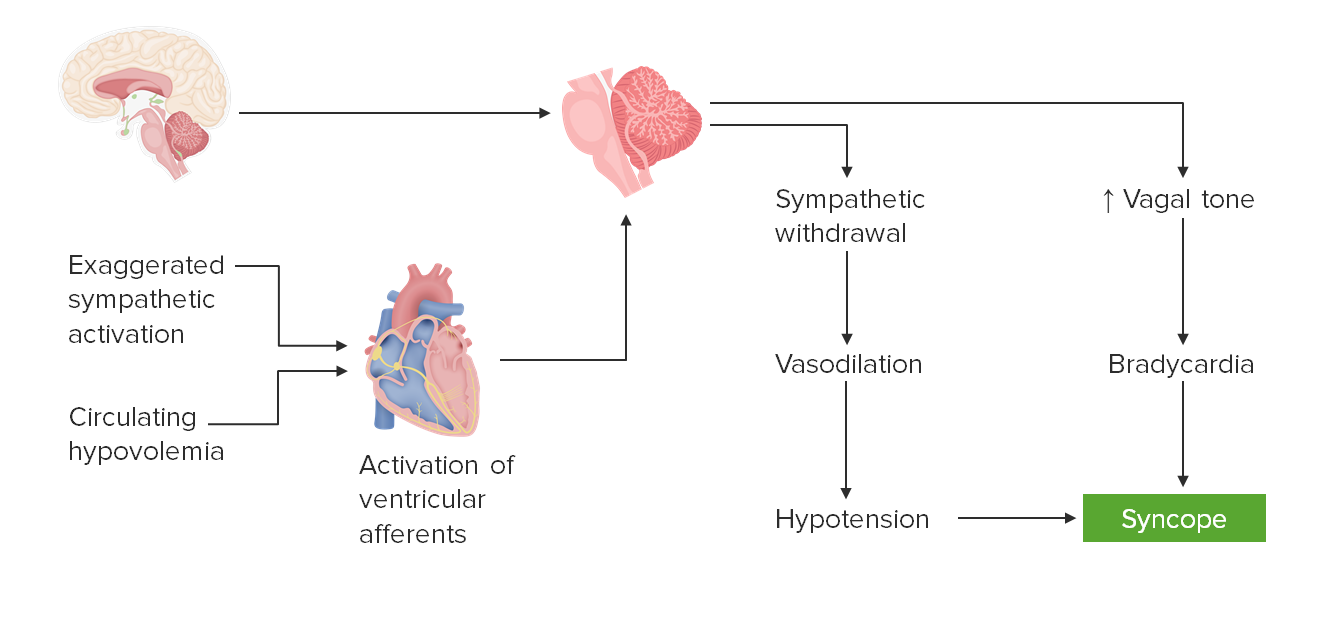
00:01 So how do we evaluate these patients who present with syncope? Well first is we need to check blood pressure and heart rate. 00:07 Both lying, sitting, and standing. 00:09 Orthostatic blood pressures are performed in the line sitting, and standing position. 00:14 And this helps us to interrogate potential problems with postural syncope or orthostasis. 00:21 And that's done through orthostatic blood pressure and heart rate. 00:23 Typically, we checked blood pressure and heart rate lying after five minutes sitting and after five minutes standing, and we're looking for a drop of 20 mmHg in the systolic pressure, 10 mmHg in the diastolic pressure without compensatory tachycardia, without an increase in heart rate by 10 beats per minute. 00:43 We can also do tilt-table testing. 00:45 This is more provocative postural testing, where we look at blood pressure, and heart rate, and cardiac rate at a range of lying positions, the table tilts. 00:56 and we can induce that postural activation that can drive some patients to syncope. 01:02 So this is a good provocative test for postural orthostatic mediated syncope. 01:07 And the neuropathy testing can be performed in some patients. 01:10 Autonomic neuropathy is a rare cause of neurally mediated syncope and neuropathic testing. 01:16 And autonomic nerve testing can be helpful in those patients. 01:21 What about the treatment? How do we treat these patients? Well, what we said was going on is either a problem with venodilation, vasodilation of vasodepressor mediated process, or bradycardia. 01:32 And that's a vaguely mediated process. 01:34 And so when we think about syncope, there's vasovagal syncope, which may be driven by problems with too little blood pressure and vagovagal syncope, which may be mediated by a reduction in heart rate. 01:47 And the final result is cerebral hypoperfusion. 01:49 But when we treat patients, we're looking to address the vaso problem and the vagal problem. 01:56 So our treatments can be divided into both of those two categories. 01:59 Our goal is to increase blood pressure and increase heart rate. 02:04 There are several things that should be avoided. 02:06 When we think about blood pressure, we want to avoid medications that reduce blood pressure like anticholinergics and antihypertensives. 02:13 When we think about increasing heart rate, we want to avoid medications that reduce heart rate like beta blockers. 02:20 At the same time, there are things we can prescribe to promote increase in blood pressure and increase in heart rate. 02:25 Hydration is the most important thing that can be done for these patients in addition to compression stockings to increase venous return to the heart. 02:33 Midodrin is an agent that stimulates increase in blood pressure. 02:36 Fludrocortisone is a medication that increases water reabsorption in the kidneys, and it can increase blood pressure. 02:43 And both of those medications can be important with the need to increase heart rate for vagovagal interventions. 02:51 And then we also think about lifestyle adjustments and lifestyle interventions to help treat these patients. 02:57 We talk to patients and counsel them on being slow to rise, when standing to be located near something where they can hold on or not jumping right up, and walking, and waiting time for their parasympathetic and sympathetic tone to balance. 03:11 Compression stockings can also be helpful for increasing venous return to the heart. 03:17 And for managing heart rate, management involves interventions to avoid situations that may induce syncope. 03:24 And this can be important for situational syncope, we avoid situations that may drive a reduction in parasympathetic and sympathetic balance.
About the Lecture
The lecture Syncope: Evaluation, Treatment, and Management by Roy Strowd, MD is from the course Vertigo, Dizziness, and Disorders of Balance.
Included Quiz Questions
Which statement is the most accurate with respect to evaluating for syncope?
- Neuropathy testing can be used to assess the autonomic nervous system.
- Orthostatic blood pressure is measured after the patient is made to sit for 10 minutes.
- A drop in systolic pressure > 5 mm Hg signifies a positive orthostatic test.
- A positive test must show both a drop in blood pressure and a drop in heart rate.
- Ain increase in systolic pressure > 5 mm Hg signifies a positive orthostatic test.
Which statement is the most accurate with respect to the treatment of syncope?
- Patients may be prescribed midodrine.
- Patients are encouraged to decrease their fluid intake.
- Patients may be prescribed anticholinergic drugs.
- Patients are encouraged to closely adhere to their antihypertensive medications.
- Patients may be prescribed beta-blockers.
Author of lecture Syncope: Evaluation, Treatment, and Management

Roy Strowd, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
