Playlist
Show Playlist
Hide Playlist
Syncope: Definition, Etiology, and Causes

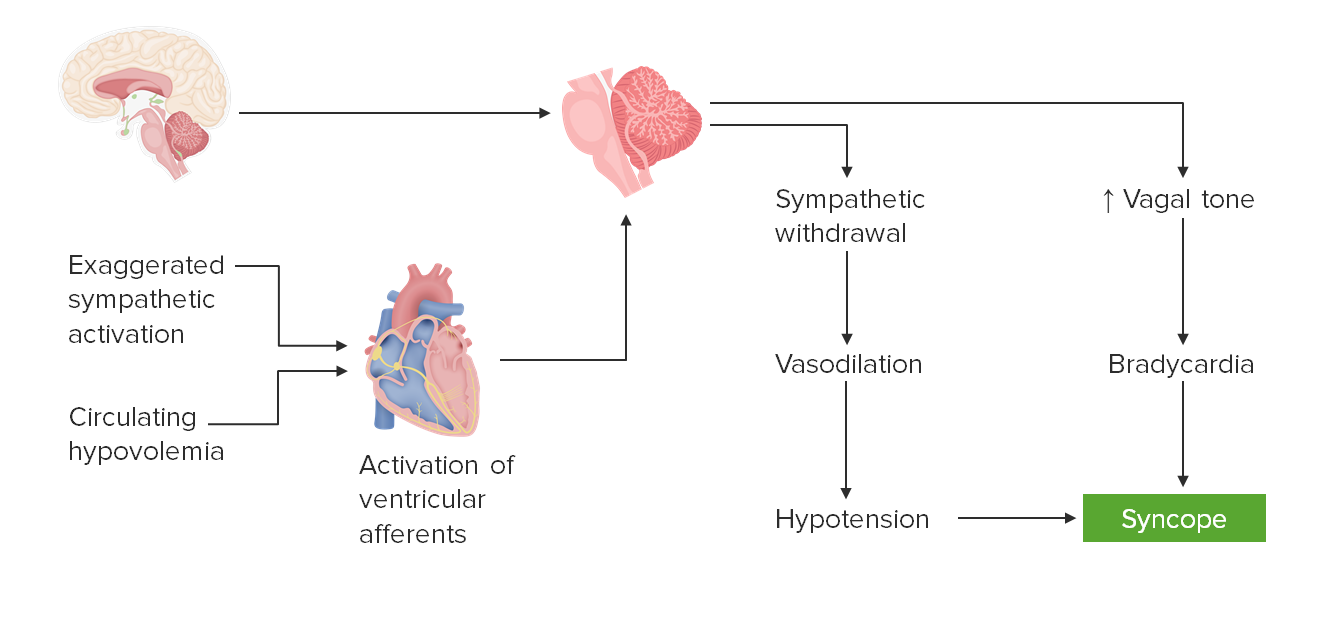
00:01 So let's talk a little bit more about syncope, and how we approach syncope? First of all, let's start with a definition. 00:07 Syncope is sudden onset of loss of consciousness, that's syncope; or near loss of consciousness, which is presyncope. 00:16 The etiology. 00:17 There are really three things that cause this. 00:20 A heart problem can cause cardiogenic syncope, reduced blood flow out of the heart. 00:26 A blood vessel problem, one of the major blood vessels like the aorta or carotid arteries can cause this problem cardiovascular or vascular related syncope. 00:36 And then the last is an issue with vascular tone, which we call neurally mediated syncope. 00:41 The blood vessels are critical for pumping blood back to the heart. 00:45 And when there's less blood pumping back to the heart, patients can pass out. 00:50 So, we'll walk through each of these three causes of syncope. 00:53 Cardiogenic syncope, syncope from a problem with the blood vessels and then an issue with vascular tone or neurally mediated syncope. 01:02 At the end of the day, the final common pathway is reduced blood flow to the brain. 01:08 And whether it be from a heart source or cardiogenic source, or a problem with the blood vessels or a vascular tone, what's going on is reduced blood flow to the brain or reduced cerebral perfusion pressure. 01:22 When blood flow is reduced to the brain, it's also reduced to the reticular activating system and the bilateral cerebral hemispheres. 01:28 And that's what keeps us awake, and thinking, and not passing out. 01:33 The reticular activating system in the brainstem lights up the bilateral hemispheres, and reduction in perfusion to any of those areas will present with presyncope or syncope. 01:45 So let's walk through each of those three causes of syncope. 01:49 And let's start with the heart or cardiogenic syncope. 01:55 The final output, the final common pathway, what's going on in patients is cerebral hypoperfusion and with cardiogenic syncope, the problem comes from the heart. 02:06 What a patient say? Patients will either describe presyncope, near fainting episodes, syncope, frank fainting episodes. 02:16 What are the causes? The cause in cardiogenic syncope is reduction in blood flow out of the heart. 02:22 That may be from a bradyarrhythmia. 02:24 The heart may be slowing down and there may be less blood, pumping out of the heart. 02:29 Patients could be suffering from heart block. 02:31 A blockage of the conduction of the electricity through the heart, and then reduced output cardiac ejection fraction. 02:39 There could be a QTc abnormality, and many of those things will be discovered on an EKG. 02:45 So when we evaluate patients, we evaluate cardiac conduction problems and ejection fraction. 02:51 We do that with an electrocardiogram. 02:54 Sometimes with prolonged ECG or EKG recording with a holter monitor or other measures to prolong monitor the heart. 03:03 And transthoracic echocardiography. 03:06 With cardiogenic syncope, the problem is reduced blood flow out of the heart because of reduction in the speed of the pumping of the heart or the amount of blood that is pumped out. 03:15 And so we evaluate those things with EKG prolonged monitoring and TTE. 03:23 What about for problems that arise from the major blood vessels? The aorta and carotid arteries. 03:28 Syncope arising from the major blood vessels. 03:33 Well, again, the final result is cerebral hypoperfusion. 03:36 Any problem that reduces blood flow up to the brain will present with syncope. 03:42 The patients in this case also describe either presyncope or syncope, just like with cardiogenic syncope. 03:49 But the causes are different. 03:51 Here we look for aortic stenosis or blockage of blood flow out of the heart. 03:56 Proximal aortic lesions like coarctation of the aorta which can be associated with a number of connective tissue diseases or neurofibromatosis. 04:05 And bilateral carotid disease. 04:07 Unilateral carotid stenosis is insufficient to generate syncope. 04:12 There's plenty of blood flow going through the opposite carotid, but bilateral carotid stenosis can present with presyncope or syncope. 04:20 That's very uncommon, but is something to be aware of. 04:24 So how do we evaluate these patients? Well, we look at each of these areas. 04:28 Carotid artery ultrasound is important for evaluating carotid stenosis and again, we're looking for bilateral carotid disease. 04:35 We do vertebrobasilar imaging either with ultrasound or a CTA, angiography of the head and neck, or even chest to evaluate the proximal aorta, and the carotid and vertebral arteries. 04:48 And then, transthoracic echocardiography is typically the first line test for evaluating aortic stenosis. 04:54 So again, problems with blockage of blood flow through the major blood vessels the aorta, or the vertebral arteries, or carotid arteries can present with syncope. 05:05 We see those descriptions from patients and we'll evaluate that on exam and diagnostic testing. 05:13 And then the last category are problems with vascular tone. 05:16 And this is coined neurally mediated syncope. 05:19 This is the most complex category of conditions that cause syncope. 05:23 And so we'll spend the most time talking about neurally mediated syncope.
About the Lecture
The lecture Syncope: Definition, Etiology, and Causes by Roy Strowd, MD is from the course Vertigo, Dizziness, and Disorders of Balance.
Included Quiz Questions
Which statement is the most accurate with regard to syncope?
- Syncope can be an indicator of a more dangerous condition.
- The underlying cause of syncope does not dictate treatment options.
- Invasive testing is the only method of determining the cause of syncope.
- Only one category of syncope results in decreased cerebral perfusion.
- The underlying cause of syncope is always related to the heart.
Which statement is the most accurate with respect to the pathophysiology of syncope?
- The heart, vessels, and neural system can all cause decreased cerebral perfusion.
- Syncope usually has a prolonged buildup and most patients experience an aura.
- Imaging studies are rarely recommended for the workup of syncope.
- Only two of the three types of syncope cause decreased cerebral perfusion.
- Increased blood flow to the reticular activating system induces sleep.
Which statement is the most accurate?
- QT prolongation can present as presyncope.
- There are no treatments for cardiogenic syncope.
- Holter monitors are diagnostic for neurally mediated syncope.
- Carotid stenosis is a cause of cardiogenic syncope.
- Ultrasound of the carotid artery can reveal neurally mediated syncope.
Author of lecture Syncope: Definition, Etiology, and Causes

Roy Strowd, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
2 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Very explicit easy understanding of the content. I have learned a lot with all this lectures.
Love the lecture and I learned a lot, looking forward to learning more!
