Playlist
Show Playlist
Hide Playlist
Surgery: Intussusception

-
Slides Intussusception Surgery.pdf
-
Download Lecture Overview
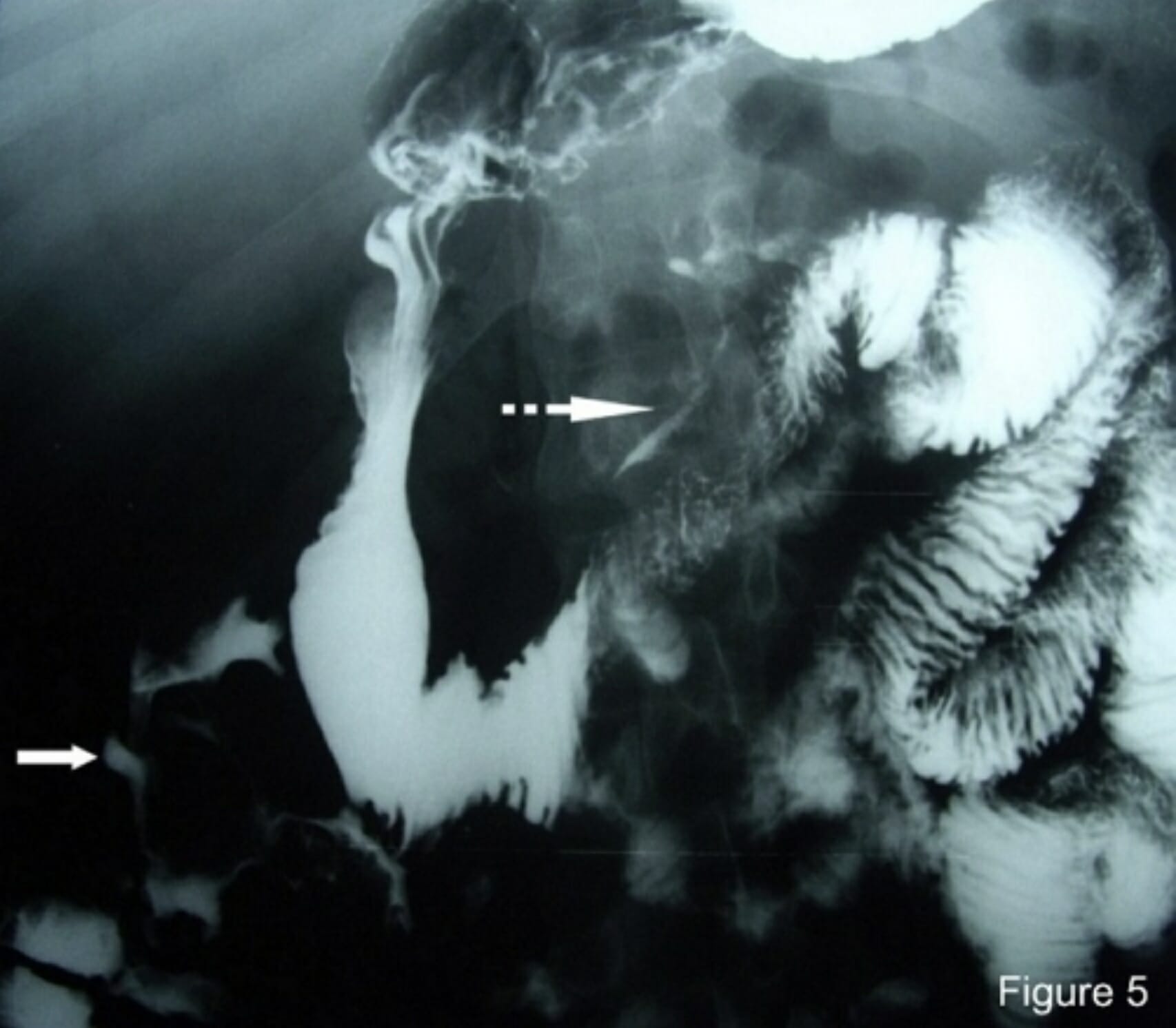
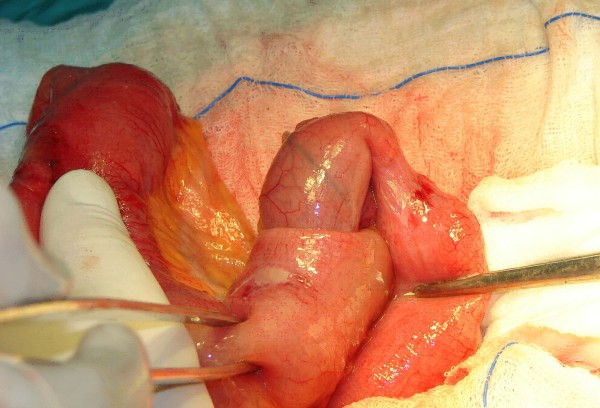
00:01 Welcome back. 00:02 Thanks for joining me on this discussion of intussusception in the section of pediatric surgery. 00:10 Intussusception, why does it happen? We don't exactly know, but there are some theories. 00:17 Most intussusception are idiopathic and they occur at the terminal ilium to the cecum. 00:23 This is also known as ileocolic. 00:26 This is the type that often happen in infants and toddlers. 00:30 Here, you see another anatomy picture of the terminal ilium actually invaginating itself into the colon. 00:39 There may be some truth behind probably lymph node hypertrophy. 00:44 Why? Because commonly this follows a recent respiratory infection. 00:50 We think with a systemic infection that the lymph nodes may actually hypertrophy and creating itself a lead point or idiopathic ileocolic intussusception. 01:03 Here is a picture of, intraoperatively, what we find in intussusception. 01:07 As you can see from this image, a segment of small intestines is invaginating into another. 01:13 This is the reason why it may cause obstruction and/or abdominal pain. 01:20 How does the intestines become ischemic during this process? I’ll show you using this image and the next few slides. 01:29 First, recognize that the lymphatic obstruction is actually what occurs first. 01:34 Commonly, when people think about intestinal ischemia, they think that the arterial supply is actually compromised first. 01:41 But there's a protective mechanism whereby the arterial blood pressure is usually the last to go. 01:47 After lymphatic obstruction, the venous side drainage is obstructed. 01:52 And now you can imagine, with lymphatics and venous obstruction, the inflow or arterial supply is subsequently obstructed. 02:01 This is like a multiple car accident. 02:04 There's going to be a pylon. 02:06 And towards the end of that scenario is arterial obstruction, and subsequently ischemia. 02:12 This is also a reason why, intraoperatively, you often see ischemic bowel very dilated. 02:17 That's because of the venous and lymphatic congestion. 02:22 Let's take a look at the schematic of what happens during an intussusception. 02:26 On the left side of the screen, as we already previously discussed, are potential etiologies of intussusception. 02:33 Remember, the vast majority of these are still idiopathic in kids. 02:37 Enlarged Peyer’s patches, particularly as associated with a viral upper respiratory infection, increases the chance of a lead point. 02:45 Additionally, some children may have an inflamed appendix, demonstrated in the left side of the screen. 02:51 As you can see on the right top half of the screen, the intestines proximally actually invaginates into the proximal small bowel. 02:59 And as a result, in the right lower quadrant of the screen, you notice that the intussusceptum, or the portion of the bowel that enters the proximal bowel, now appears edematous. 03:10 Upstream of this edematous bowel can present with small bowel obstruction. 03:15 As you can imagine, when venous and lymphatic drainage is obstructed, it may need to ultimately arterial obstruction and subsequent bowel ischemia. 03:25 Remember, lead points may not always be present.
About the Lecture
The lecture Surgery: Intussusception by Kevin Pei, MD is from the course Special Surgery.
Included Quiz Questions
What is the CORRECT sequence of vessel obstruction in cases of intestinal ischemia resulting from intussusception?
- Lymphatic obstruction, venous obstruction, arterial obstruction
- Lymphatic obstruction, arterial obstruction, venous obstruction
- Arterial obstruction, lymphatic obstruction, venous obstruction
- Arterial obstruction, venous obstruction, lymphatic obstruction
- Venous obstruction, arterial obstruction, lymphatic obstruction
Which of the following is the most common location of intussusception in infants?
- Ileocolic
- Colocolic
- Ileo-ileo-colic
- Ileoileal
- Retrograde
Author of lecture Surgery: Intussusception

Kevin Pei, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
