Playlist
Show Playlist
Hide Playlist
Gastrinoma

-
Slides gastromina General Surgery.pdf
-
Download Lecture Overview
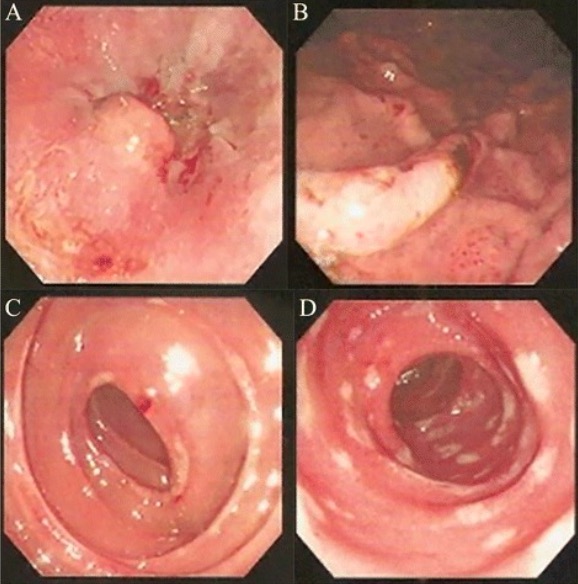
00:01 Welcome back. Thanks for joining me for this discussion of gastrinomas in the section of general surgery. 00:09 Gastrinomas result in gastric acid hypersecretion. As a result, patients can develop severe and debilitating acid-related peptic ulcer disease. Remember, when a clinical scenario is presented to you that has difficult to treat ulcer disease, think gastrinoma. Gastrinoma results in the secretion of gastrin by duodenal or pancreatic gastrinomas. As a result of the high gastrin levels, there is increased gastric acid secretion. Here’s a depiction of mechanism of action of gastrin. Gastrin stimulates increased histamine release through the enterochromaffin like cells or ECL. This is highlighted in the yellow box. As a result of increased histamine production, the parietal cells then increase acid secretion. Note however, that acid is actually a negative feedback on gastrin levels. 01:11 Our bodies have control mechanisms in place so that with increasing acid or decreasing pH levels, the G cells actually reduce our gastrin secretion. In patients who have gastrinomas Where this acid cannot provide the negative feedback to the G cells, we actually have a hypergastrinemia. 01:35 What are some physical findings associated with gastrinomas? Patients often complain of diarrhea. 01:41 Here’s also a picture of severe peptic ulcer disease. As a reminder, any peptic ulcer disease, that is difficult to treat once you consider gastrinoma. The etiology of the diarrhea actually comes from high acid, low pH’s ability to inactivate pancreatic enzymes which are necessary for fat absorption. As a result of this decreased pancreatic enzyme activity, poor fat absorption leads to fatty stools and diarrhea. Historically, patients may complain of weight loss, GI bleeding again associated with a difficult to treat peptic ulcer disease, and as a reminder, the very high-yield multiple endocrine neoplasia particularly type 1. 02:35 Here you have the different forms of multiple endocrine neoplasia type 1 in an high-yield overview. 02:41 Type 1 multiple endocrine neoplasia involves parathyroid tumors, pituitary tumors, and pancreatic tumors. 02:47 They are including gastrinomas, insulinomas which are discussed in a different module, VIPoma and Glucagonoma. 02:54 Routine laboratory studies are unlikely to be helpful including chemistries and CBCs. 03:01 However, unique to gastrinomas is a plasma gastrin level. 03:06 Values greater than 1,000 pg/cc is considered significant and almost diagnostic of gastrinoma. 03:15 Similarly, an adjunctive secretin stimulation test can also demonstrate a gastrinoma by a paradoxical increase in the gastrin level. 03:26 Some imaging study may be helpful in diagnosis or localizing the gastrinoma. 03:33 This image demonstrates a cross-sectional CT scan abdomen/pelvis demonstrating a duodenal or head of the pancreas mass. 03:39 In the appropriate clinical setting, this may represent a gastrinoma. Remember, gastrinomas are not limited to pancreas. 03:46 It can also occur in the duodenum. Medical therapy of gastrinomas includes proton pump inhibitors. 03:56 Unfortunately, because of the continued gastrin secretion, proton pump inhibitors may provide only transient symptomatic relief. 04:05 Unfortunately, the vast majority of patients with gastrinoma will require a surgical resection. 04:11 Let’s assume that the mass was in the duodenum. In this situation, the entire duodenal area and including the head of the pancreas may need to be resected with subsequent reconstruction. 04:24 This is the depiction of a pancreaticoduodenectomy or a classic Whipple procedure. 04:30 In some instances when the gastrinoma is in the head of the pancreas or even in the duodenum, common tiers of blood supply mandates that all surrounding tissues be removed. 04:41 As a result, multiple reconstructions have to be recreated such as a hepaticojejunostomy, a pancreaticojejunostomy, and ultimately a gastrojejunostomy. Every pancreaticoduodenectomy has three anastomoses. 04:57 Here's a clinical pearl to remind you of. 05:01 When a patient has a difficult to treat peptic ulcer or peptic ulcer that is not responsive to medical management, or peptic ulcers beyong the first part of the duodenum, consider gastrinoma in your differential diagnosis. 05:11 For your examination, it’s also worthwhile to discuss Zollinger Ellison syndrome. 05:19 Zollinger Ellison syndrome is a syndrome related to gastrinomas or hypergastric acid secretion. 05:26 This is the classic triad of peptic ulcer disease, diarrhea, and high gastrin levels. 05:32 Again, presenting symptoms include abdominal pain, diarrhea from the poor fat absorption, and heart burn, chronic in nature. 05:43 This may be associated with an MEN syndrome, typically MEN type 1: parathyroid, pituitary, and pancreatic lesions. 05:53 Thank you very much for joining me in this discussion of gastrinomas.
About the Lecture
The lecture Gastrinoma by Kevin Pei, MD is from the course General Surgery.
Included Quiz Questions
Which types of tumors are NOT typically associated with MEN 1 Syndrome?
- Pineal gland tumors
- Pituitary tumors
- Pancreatic gastrinomas
- Pancreatic insulinomas
- Parathyroid tumors
Which of the following statements about gastrinomas is FALSE?
- Gastrinomas secrete gastric acid
- Gastrinomas stimulate enterochromaffin-like cells
- Gastrinomas result in fatty diarrhea
- Gastrinomas are associated with MEN 1 syndrome
- Gastrinomas are typically found in the head of the pancreas and the duodenum
A 58-year-old woman presents with persistent epigastric abdominal pain despite high-intensity proton-pump inhibitor therapy for gastric ulcer disease. She is unable to eat full meals due to debilitating abdominal pain, has frequent fatty stools, and has unintentionally lost about 15 pounds in the past 4 months. You order labs and note that plasma gastrin levels are elevated. What is the most likely diagnosis?
- Zollinger-Ellison Syndrome
- Advanced peptic ulcer disease
- Exogenous administration of histamines
- Gastric parietal cell tumor
- Gastric carcinoma
A patient with persistent peptic ulcer disease, fatty diarrhea, and weight loss is found to have a gastrinoma in the duodenum. Which treatment can be curative?
- A pancreaticoduodenectomy (Whipple procedure)
- Resection of the head of the pancreas only
- Resection of the duodenum only.
- High dose proton-pump inhibitor and anti-histamine treatment
- Gastric resection
Author of lecture Gastrinoma

Kevin Pei, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
