Playlist
Show Playlist
Hide Playlist
Summary of Membranoproliferative Glomerulonephritis (MPGN)



-
Slides MembranoproliferativeGlomerulonephritis RenalPathology.pdf
-
Reference List Pathology.pdf
-
Download Lecture Overview
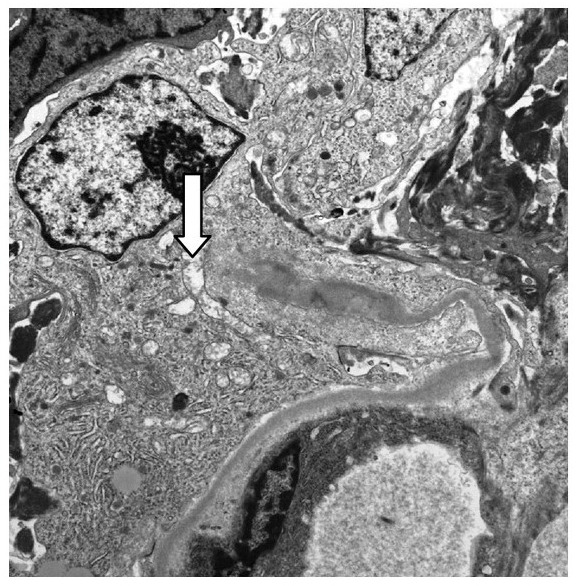
00:01 Thickening at the basement membrane with MPGN, formation of tram-track either type I or type II, can be primary or secondary. 00:08 Immune complex will be the most common. 00:11 That will be type I as we have discussed. 00:13 CLL, lymphoma, melanoma. 00:16 All of these, once again, associations. 00:18 Clinical features could be nephritic, nephrotic, or mixed. 00:22 Decrease serum C3, much more so with type II. 00:26 Prognosis, slowly progressive course. 00:29 Many of your patients within 10 years will go into chronic renal failure. 00:34 Overall picture of MPGN. 00:36 Where do you begin your biopsy and pattern differentiation? At the level of electron microscopy. 00:42 Know the flow chart well that I showed you earlier between the two. 00:45 Know the details that we walk through here, with type I and type II. 00:50 Type I, sub-endothelial, striking tram-track. 00:54 Type II, dense deposit disease. 00:57 Nephritic factor, what does it do? It then causes stabilization and deposition, less striking tram-track but both will have it. 01:06 Clinically characterized by, decrease levels of C3, type II complement mediated damage. 01:14 On your upper left in the cartoon, type I sub-endothelial, type II intramembranous. 01:22 That intra membranous, upon electron microscopy, will then show you dense deposit disease. 01:27 The one on your left represents sub-endothelial. 01:33 Let’s do the pattern organization. 01:35 I don’t wanna get away from that. 01:36 Number one, find the pave road. Where is it? You see that light gray paved road in the membrane? That’s your glomerular basement membrane. 01:49 I would like for you to find feet. 01:52 The feet are on top, that’s your foot processes. 01:57 So that’s the urinary side, upper right. 02:00 Lower side, you’ll find that huge, dark, density? That’s your sub-endothelial deposit, type I. 02:08 You see that membrane? Yeah, Dr. Raj. 02:12 But that looks awfully dark to me? That’s the pathology. Clear? That’s dense deposit disease. That’s type II. 02:19 Where’s the CL? That would be capillary lumen. But who cares? The reason I say that is because it’s deposition of dense amorphous material in your membrane. 02:27 Welcome to type II. 02:30 Can you give me the pathogenesis here. Nephritic factor. 02:34 What does that do? Destroy or stabilize C3 convertase. 02:39 Do you remember? Do you hear my terminology? It stabilizes C3 convertase. Good. Intense. 02:45 But you have to know at least that much to get your questions right.
About the Lecture
The lecture Summary of Membranoproliferative Glomerulonephritis (MPGN) by Carlo Raj, MD is from the course Glomerulonephritis.
Included Quiz Questions
Which of the following best describes the pathogenesis of Type II membranoproliferative glomerulonephritis?
- Dysregulation of the alternative complement pathway
- Overactivation of the classical complement pathway
- Monoclonal gammopathy with decreased clearance
- Overproduction and decreased clearance of IgA
- T-cell cytokine mediated damage of podocytes
How is type 2 membranoproliferative glomerulonephritis characterized clinically?
- Decreased levels of serum C3
- Hypogammaglobulinuria
- Decreased levels of serum C3bBb
- Elevated levels of serum IgA
- Hypoalbuminuria
What clinical manifestation would you expect most commonly in a patient with either type I or type II membranoproliferative glomerulonephritis?
- Hematuria
- Hypotension
- Bleeding diathesis
- Fever
- Oliguria
How would the biopsy of membranoproliferative glomerulonephritis be described?
- Thickening of basement membrane with the proliferation of mesangial cells
- The linear pattern on immunofluorescence
- The proliferation of parietal epithelial cells on light microscopy
- Subepithelial deposits on electron microscopy
- Damage of visceral epithelial cells on electron microscopy
Which of the following statements about membranoproliferative glomerulonephritis is INCORRECT?
- Type 1 and Type 2 may be differentiated by light microscopy.
- Less than half of patients present with hypertension.
- Response to corticosteroids is not established.
- Majority progress to CRF.
- Majority of patients present with hematuria.
Which of the following is characteristic of type 2 MPGN?
- Irregular dense deposits within GBM with adjacent C3
- Increased levels of serum C3
- Decreased levels of serum C4
- C3 nephritic factor that destroys the C3 convertase
- Elevated levels of IgA
Which of the following is associated with type 2 MPGN?
- Diffuse intramembranous deposits
- Subendothelial immune complex deposits with granular immunofluorescence
- Diffuse thickening of the membrane with subepithelial immune complex deposits
- Mesangial IgA immune complex deposits
- Fusion of podocytes
Author of lecture Summary of Membranoproliferative Glomerulonephritis (MPGN)

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
