Playlist
Show Playlist
Hide Playlist
Subdural Hematoma: Etiology and Clinical Presentation

-
Slides Head Trauma Subdural Hemorrhage.pdf
-
Download Lecture Overview
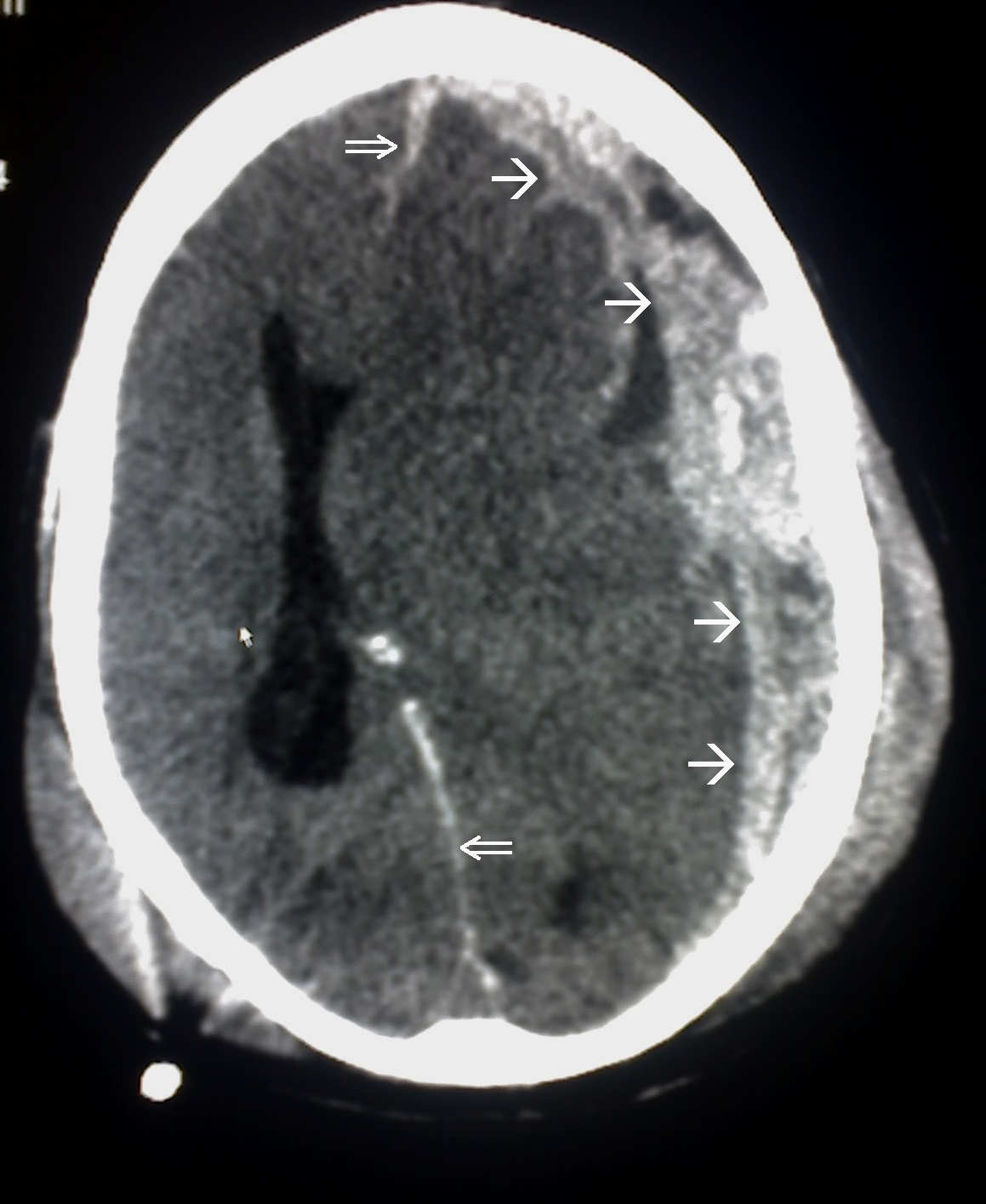
00:01 So let's talk a little bit more about subdural hematomas. 00:04 And let's start with a definition. 00:06 Subdural hemorrhage or subdural hematoma is a bleeding event into the space between the dura and arachnoid meningeal layers surrounding the brain. 00:15 So let's look at that at what's happening in this schematic. 00:18 And again, we're looking at the bones and the skull going down to the parenchyma of the brain. 00:24 With a subdural hemorrhage, the problem is in the subdural space. 00:28 In between the dura and the arachnoid mater over the surface of the brain. 00:34 Here we see blood layering over the surface of the brain in a crescent shape that extends beyond suture lines. 00:41 And that differs from the imaging appearance of epidural hematomas. 00:46 In terms of epidemiology, this is typically found as a result of head trauma and 10% of head trauma is necessitating hospitalization. 00:56 It's found in 20% of severe traumatic brain injury patients. 01:00 More common in older individuals, and we'll talk about why that may be and more common in persons who are on antiplatelet or anticoagulant therapies. 01:08 And so those are potential risk factors for the development of a subdural. 01:14 So let's talk about the etiology. 01:16 Subdural hematomas most commonly occur as a result of a fall. 01:20 The fall causes injury to vascular structures that course between the dura and the arachnoid layers and we'll talk about why that is. 01:30 This most commonly exerts forces in the anteroposterior direction. 01:33 So anteroposterior forces and trauma lead to injury to the bridging veins that are in that subarachnoid and subdural space and can result in the development of a subdural hemorrhage. 01:46 And examples of such trauma include motor vehicle accidents, falls and assaults. 01:52 So let's look at what's happening, pathophysiologically, what's causing the development of a subdural? So first, let's look at what's happening in the setting of tearing of bridging veins. 02:02 And here we're looking at a coronal schematic of the brain. 02:06 We have the bones at the top, we have this dural reflection at the sinus and we see outside of the sinus extending into the brain of the veins and they help to drain the brain of blood supply. 02:19 These bridging veins are susceptible to tearing in the setting of anteroposterior trauma. 02:25 These veins connect the brain to the superior sagittal sinus. 02:30 They traverse the space in between the arachnoid and the dural meningeal layers. 02:35 And as a result of tearing from trauma, this allows blood to collect in between those two layers in the subdural space. 02:45 Bleeding may be occluded by rising intracranial pressure or direct compression by the developing thrombus. 02:54 This most commonly is observed in the temporal parietal regions, but we can see subdural hematomas anywhere in the brain. 03:02 We can also see subdural is develop as a result of arterial rupture, which is less common but can be more concerning. 03:08 And again, we have those arteries extending between the dural reflections in the brain itself. 03:14 Small arteries or arterioles are often less than one diameter as they coursed through this area. 03:21 They supply blood to the superficial cerebral cortex. 03:24 They provide the collaterals that help to collateralize that area of cell bodies. 03:29 They traverse the space between the arachnoid and the dura and so they're susceptible to tearing as a result of trauma. 03:36 And as a result of rupture, we see blood developing in that subdural space. 03:40 And again, tamponade of bleeding may occur from rising intracranial pressure as the blood expands, or by thrombus compression as it develops in these layers. 03:54 So what's the clinical presentation of a subdural? Well, acute subdural is present immediately, often within 72 hours of the traumatic event. 04:03 The initial presentation is either with focal neurologic deficit or coma in half of cases. 04:08 And many patients will have slow and steady progression of symptoms over time, which differentiates subdural cells from that epidural hematoma presentation where we may see a lucid interval. 04:20 Subacute subdural s can also occur as a result of slow accumulation of blood over time or with repeated traumas in elderly patients where there's particular repeat tearing up those bridging veins and may present three to 14 days after the event. 04:35 Subacute subdural is appear as less hyper dense or with mixed density on the CT. 04:40 And chronic subdural is can also be a contributing factor to clinical presentations presenting more than 15 days after the event. 04:47 And as they're slow expansion of that blood over time, this can result in symptoms. 04:51 And typically, this blood will appear isointense to the brain and not have that hyperdense appearance on CT. 04:59 In terms of neurologic symptoms, the nature of the symptoms like epidural hematomas depend largely on four characteristics. 05:06 1. Where is the hematoma? The patient's symptoms will differ depending on where the hematoma occurs. 05:11 What is the size? Larger hematomas are gonna result in more increases in ICP, and smaller hematomas may be asymptomatic or simply affect the cortex underlying where the hematoma is. 05:22 The rate of growth will determine the speed at which the patient's neurologic deficits occur and the acuity of the trauma may also contribute to the patient's symptoms. 05:30 So we look at all four of these findings and signs. 05:33 When we're understanding how we manage the patient and the symptoms or signs that they may present with. 05:41 Some of the common symptoms we see are altered level of consciousness. 05:44 Minor trauma may result in momentary loss of consciousness or more severe trauma into coma. 05:50 Subacute and chronic subdural may result in very gradual deterioration over time. 05:55 We can see headache, lightheadedness, dizziness, neck pain or stiffness, visual changes, nausea, vomiting from increased ICP balance or gait dysfunction or dysphagia. 06:05 Pretty much any symptom can develop in these patients depending on where the hemorrhage is and the degree of increase in ICP. 06:12 Other common signs we may see on exam is nuchal rigidity. 06:16 This blood is in that subdural space and we can say some irritation of the cortical surface and of the meningeal layer. 06:22 Cranial nerve palsies may occur, ataxia may develop, and seizures can occur in some of these patients, though not all.
About the Lecture
The lecture Subdural Hematoma: Etiology and Clinical Presentation by Roy Strowd, MD is from the course Head Trauma.
Included Quiz Questions
What is the term for bleeding between the dural and arachnoid meningeal layers around the brain?
- Subdural hematoma
- Epidural hematoma
- Subarachnoid hemorrhage
- Intraparenchymal hemorrhage
- Intraventricular hemorrhage
What is the most common etiology of subdural hematomas?
- Falls
- Motor vehicle accidents
- Blunt force injuries
- Blast injuries
- Whiplash injuries
Which vascular structure is most often implicated in subdural hematomas?
- Bridging veins
- Middle meningeal artery
- Circle of Willis
- Dural venous sinuses
- Posterior cerebral circulation
In a patient presenting after head trauma with a lucid interval and resultant coma, what clinical factor gathered from the history might help distinguish an acute subdural hematoma from an epidural hematoma?
- Length of the lucid interval
- Presence of focal neurologic deficit
- Presence of headache
- Mechanism of motor vehicle accident
- Smoking history
Author of lecture Subdural Hematoma: Etiology and Clinical Presentation

Roy Strowd, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
