Playlist
Show Playlist
Hide Playlist
Stomach Tumors

-
Slides Stomach tumors General Surgery.pdf
-
Download Lecture Overview
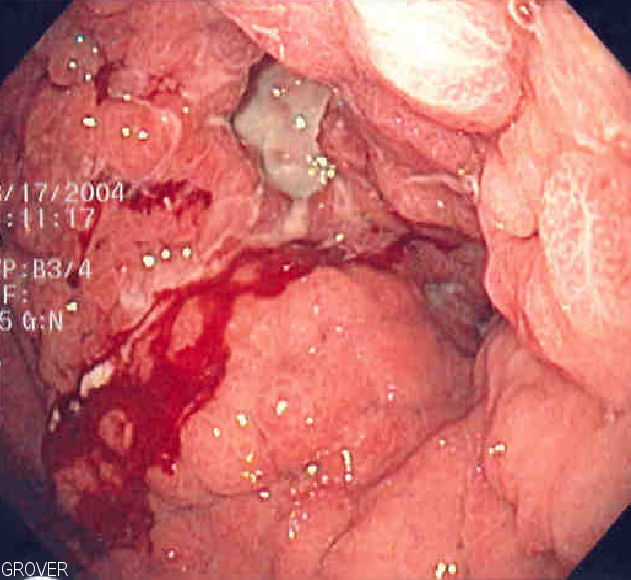
00:01 Welcome back. Thanks for joining me on this discussion of stomach tumors in this section of general surgery. 00:07 Let’s begin the discussion about gastric adenocarcinoma. There are some risk factors that are classically associated with gastric adenocarcinoma. They include low fiber diets, Helico pylori infection, chronic gastritis, nitrosamines and preserved foods. This is an important slide giving you three particular findings that are consistent with advanced metastatic stomach cancer. One is Virchow's node which is a supraclavicular lymph node; Sister Mary Joseph sign, which is a periumbilical lymph node; and Blumer's shelf palpable nodule in the rectal vault when you do a rectal examination. Again, all three findings are suggestive of advanced adenocarcinoma. What are some signs and symptoms of gastric adenocarcinoma? In its late stages, one can find weight loss, early satiety, and anemia. 01:14 Weight loss is not completely understood but in most oncologic processes, weight loss has something to do with the tumor necrosis factor, TNF. Early satiety may be due to a mass effect or simply again, an oncologic syndrome. Anemia may be due to chronic slow bleeding that is subclinical. 01:34 Meaning, it hasn’t caused the patient low blood pressure. What are specific findings and laboratory indicative of adenocarcinoma? Not a lot, routine chemistries may be very normal. 01:48 Again, a drop in the hemoglobin or hematocrit may be a very late finding. The vast majority of patients with particular history of gastritis have undergone H. pylori testing. Here’s an upper endoscopy with biopsies demonstrating a large fungating mass in the stomach. Endoscopic ultrasound, as demonstrated on this image is a very modern technique of demonstrating particularly proximal stomach or distal esophagus cancers. The depth of penetration of any GI system cancer is very, very important. Endoscopic ultrasound can help us determine the depth of penetration. 02:30 After diagnosing somebody with a stomach cancer, the next step is to perform a metastatic workup. 02:40 This again can include a CT scan cross sectional imaging of the abdomen and pelvis. In this CT scan, the black arrow demonstrates multiple sites of metastases from stomach cancer. Just a reminder, just because one finds multiple lesions in the liver doesn’t mean that it’s necessarily metastasis. 03:00 In any clinical scenario, it’s important to have context. So, if you suspect given the presentation of a patient with stomach cancer or any cancer for that matter and you see multiple lesions in the liver, the most likely diagnosis is a liver metastasis as opposed to primary liver cancer. After diagnosing somebody with stomach cancer and doing the metastatic workup, deeming the patient "resectable" then we offer the patient a gastrectomy. A gastrectomy whether it’s subtotal, meaning removing just about the entire versus a total gastrectomy depends on the position of the cancer. 03:42 Proximal tumors or tumors close to the esophagus are treated with a total gastrectomy as opposed to distal stomach cancers are usually treated with a subtotal gastrectomy. 03:54 The reconnections can be complicated and are beyond the purview of this course. 04:01 A special scenario which is high yield in nature are mucosal associated lymphoproliferative tissue, also known as MALTOMAs. MALTOMAs are very important as a distinction from gastric adenocarcinoma because this is generally a low grade B cell lymphoma of the mucosa and is associated with lymphoid tissue. 04:24 The treatment however is vastly different. The treatment does not include surgery, rather, it is by simply eradicating H. pylori. This is an important message. When you suspect the patient of a B cell lymphoma or MALTOMA of the stomach, treatment is not surgery. 04:41 Again, it’s simply eradication of H. pylori infection. An important clinical pearl: Diseases may present at a very advanced stage given the insidious symptoms. So, to remind you, bleeding, weight loss, early satiety are generally late cases and patients have already presented with advanced disease. 05:04 Thank you very much for joining me in this discussion of stomach tumors.
About the Lecture
The lecture Stomach Tumors by Kevin Pei, MD is from the course General Surgery.
Included Quiz Questions
Which of the following is not considered a risk factor for gastric adenocarcinoma?
- Acute gastroenteritis
- Low fiber diet
- Helicobacter pylori infection
- Chronic gastritis
- High nitrosamine diet
All of the following are indicative of advanced metastatic gastric adenocarcinoma EXCEPT?
- Enlarged internal mammary lymph node
- Virchow's node
- Sister Mary Joseph nodule
- Blumer's shelf
- Left supraclavicular lymph node enlargement
How is esophageal ultrasound a useful tool in diagnosing and staging gastric adenocarcinoma when compared with endoscopy?
- It allows for visualization of the depth of penetration of the tumor.
- It allows for the visualization of distal gastric tumors.
- It is superior to upper endoscopy in identifying areas of tissue necrosis.
- It allows for the identification of metastases.
- It can be used to cauterize bleeding gastric tumors during evaluation.
What is the treatment for mucosal-associated lymphoproliferative tissue gastric cancer (MALToma)?
- Eradication of Helicobacter pylori infection
- Total gastrectomy
- Subtotal gastrectomy
- Chemotherapy
- Radiotherapy
A 58-year-old man with a past history of Helicobacter pylori treatment failure and chronic gastritis presents to the outpatient clinic with progressive symptoms of decreasing appetite, early satiety, and weight loss. He states that he can’t even enjoy his favorite food, canned meat, anymore. On exam, you note that he is thin, pale, has a soft, non-tender abdomen, and has a palpable smooth, mobile mass near his umbilicus. What is most concerning about this presentation?
- This patient has signs of advanced gastric adenocarcinoma
- This patient has early gastric adenocarcinoma, as his symptoms are still quite mild
- This patient likely has significant anemia and needs to receive blood transfusions for stabilization
- This patient has an incarcerated umbilical hernia which must be operated on urgently
- This patient needs repeat treatment for Helicobacter pylori, as he is showing signs of increased proliferation of the bacteria
Author of lecture Stomach Tumors

Kevin Pei, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Everything is explained carefully, nicely, slowly, and there's no false information
