Playlist
Show Playlist
Hide Playlist
Status Epilepticus: Stages and Pathophysiology

-
Slides Seizures Epilepsy Status Epilepticus.pdf
-
Download Lecture Overview
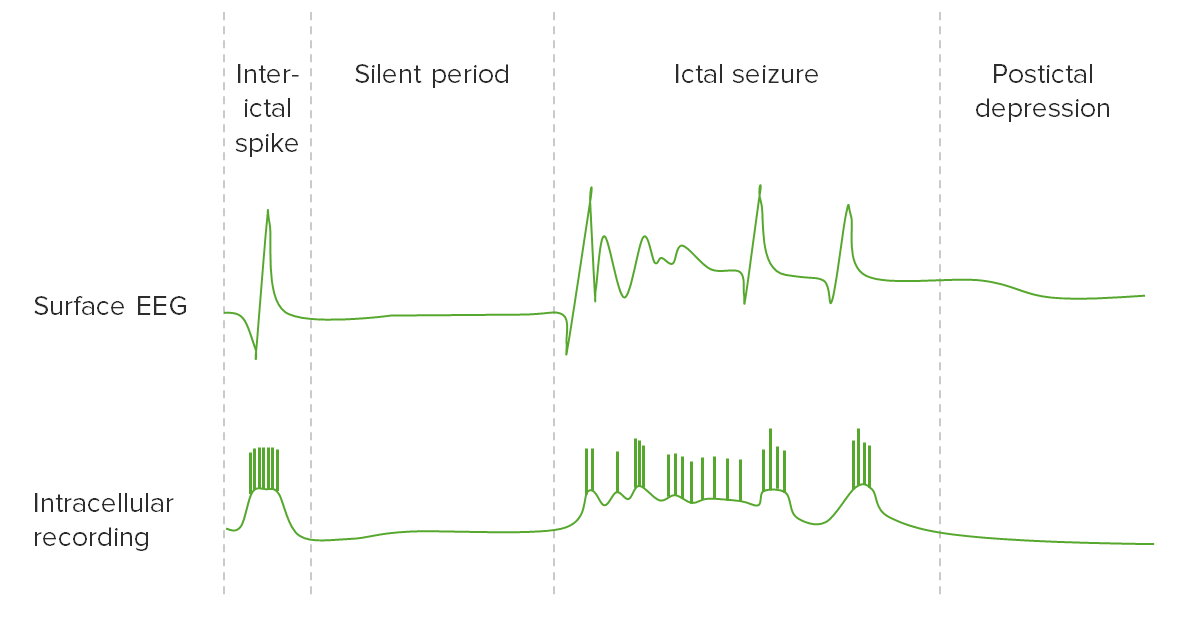
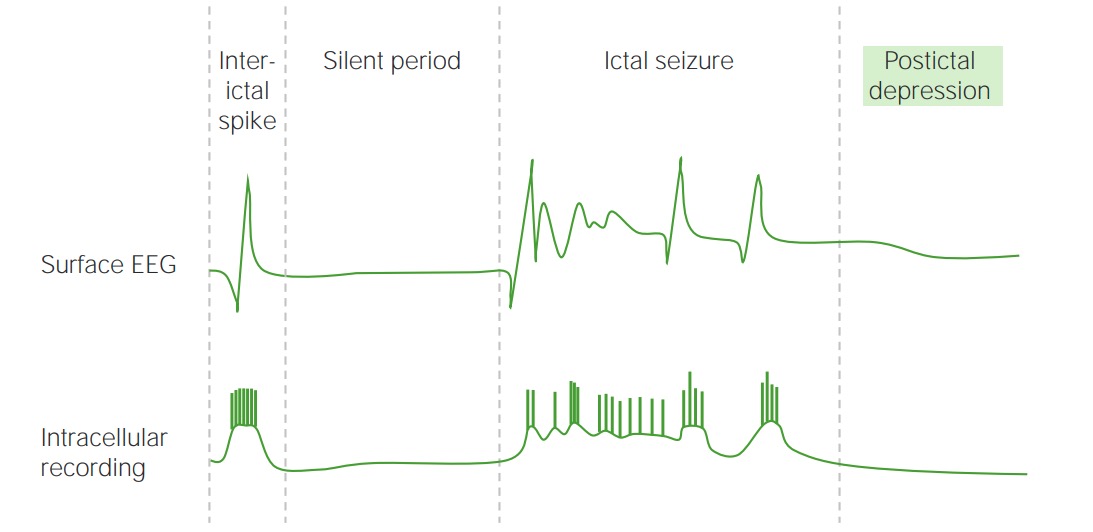
00:01 When we think about status and that treatment algorithm, the status presents in stages as we look at treating through these stages. 00:09 There's the premonitory phase, where patients may have confusion, myoclonus, or increased seizure frequency. 00:15 And that's happening right before this continuous seizure activity develops. 00:19 And there may be discrete ictal activity that can be seen on the EEG during this period of time. 00:25 This gives rise to the incipient phase the first 0 to 5 minutes, when that seizure is occurring. 00:31 When we're looking at stabilizing the patient, we see frequent seizure activity and waxing and waning of ictal activity on the EEG. 00:39 In the early portion of status the first 5 to 30 minutes there is continuous seizure activity, both clinically and we see that with continuous ictal discharges on the EEG. 00:49 Late we can see that sometimes the seizure activity will burn out during that 30 to 60 minutes of prolonged seizure activity. 00:56 Clinically, the patient may have continuous seizure activity and continuous ictal discharges. 01:01 And we may start to see that continuous clinical activity break up as well as some flat periods on the EEG, as the brain becomes overrun by the status, and some of those nutrients that we talked about in the pathophysiology start to be depleted. 01:16 Ultimately, in refractory cases where seizures last longer than 60 minute, we see convulsive status morphin progress into subtle convulsive status or nonconvulsive status epilepticus. 01:28 We lose the motor activity, clinically, and sometimes we can lose that continuous spike and wave activity with periods of flattening on the EEG. 01:36 We can see periodic epileptiform discharges with a flat background in the middle. 01:41 And those all indicate a more progressed and refractory status epilepticus, which is harder to treat and associated with a poor prognosis. 01:49 As we think about the stages of status and move further away from the acute stabilization to long-term management of status. 01:56 Stage 1 was the early phase, that premonitory and impending status epilepticus. 02:01 Stage 2 is the established status epilepticus that first 30 to 60 minutes when we're evaluating the patient, when we're intervening, giving definitive seizure management, and trying to rescue the patient from further progression of the status. 02:16 Patients who do not respond to one and then two definitive seizure treatments, and a refractory to definitive seizure management of status epilepticus move into stage 3. 02:27 Stage 3 is classified as refractory status epilepticus. 02:31 That status that continues despite stage one or two treatment. 02:35 Progresses after the benzodiazepine abortion and after two definitive seizure medications. 02:41 Oftentimes, we'll see patients progress to subtle status epilepticus, nonconvulsive status epilepticus, or a stuporous status epilepticus during that phase. 02:50 This is treated with high dose intravenous antiepileptics. 02:53 Often patients are put into the ICU intubated and put into a burst suppression, where the medications are titrated to a level that the brain almost becomes very flat and attenuated. 03:05 At that stage, patients are kept in a burst depressions pattern for about 24-hours, to try and reset the brain to stop the brain from remembering how to have continuous seizure activity and aborting the status epilepticus. 03:20 Seizures that continue after that stage three intervention are considered super-refractory. 03:26 And those patients with super-refractory status epilepticus have continuous seizure activity, despite the use of anesthetics for 24-hours. 03:34 And that stage 4 becomes very difficult to treat and with this extremely poor prognosis. 03:41 So let's walk through the pathophysiology of what's happening in the brain during those stages, so we can understand how we're going to manage patients in the importance of early intervention. 03:51 Again, we considered the acute seizure, the early status epilepticus, and then we'll talk about what's happening in the brain during these refractory and malignant status epilepticus phases. 04:03 Let's start by thinking of the neurophysiology. 04:05 During the acute seizure and early status phase, we see receptor trafficking. 04:11 There's reduced GABA tone and increase release of NMDA, and glutamate. 04:16 Less inhibitory tone and more excitatory tone, and those are building in the brain during that early acute seizure and status epilepticus period. 04:25 Ultimately, this transitions into synaptic plasticity. 04:29 Changes in the way the synapse looks, and biochemically communicate. 04:34 There's modification of the GABA receptor and composition and this drives further seizure activity. 04:41 seizures, begetting seizures. 04:44 What about in terms of the motor activity? What do we see in the patient? Well, early for convulsive status, we see generalized convulsions, both with the acute seizure and the early status epilepticus. 04:56 Over time, those generalized convulsions that jerking back and forth of the body peter out into myoclonus. 05:03 And we see less motor activity as the brain and the motor system become overrun by the continuous seizure activity. 05:11 And ultimately we can see electromechanical dissociation, where the body is jerking, but it doesn't line up with the epileptiform discharges that we see on the brain. 05:22 And that's seen in these severe and refractory cases. 05:26 How about systemic pathology? What's going on systemically? First, we see in the early acute seizure and early status epilepticus phase, a compensatory phase there is sympathetic overdrive. 05:38 the heart will speed up and there's increased sympathetic tone as the body tries to compensate for the continuous seizure activity. 05:46 This gives way to decompensation and homeostatic failure, and we can start to see organ dysfunction in patients who have had significant status for a prolonged period of time. 05:57 Some of the things that we see in the compensatory phase are increased cardiac output, increased blood pressure, increased blood glucose, and increased blood lactate. 06:06 The body is trying to support the brain through the seizure activity by increasing things like ejection fraction, cardiac output, and glucose. 06:14 Ultimately, those compensatory mechanisms fail with prolonged seizure activity. 06:19 Cardiac output may decline, blood glucose may go down, as glucose is depleted. 06:23 Blood lactate may decline, and blood oxygen may decline. 06:26 And so you can start to see some of the potential reasons why we see multi organ failure in patients with long term status epilepticus. 06:34 Ultimately, in most of your cases, Cardiorespiratory collapse can occur, electrolyte imbalances, hyperthermia, as a result of temperature dysregulation. 06:43 Rhabdomyolysis from the continuous motor activity and delayed tubular necrosis or damage to the kidneys as a result of that. 06:50 And ultimately, in severe cases, again, multi organ failure. 06:54 So this is emergency. 06:56 We must act quickly to stop this situation before those complications develop. 07:01 How about brain metabolism? What's going on in the brain during status? We initially see, sometimes increases or stabilization of cerebral blood flow as autoregulation kicks in to maintain blood flow during this event. 07:13 We see glucose and oxygen are sufficiently where they should be normal glucose and oxygen in the brain, as well as brain tissue oxygenation, and brain glucose. 07:24 And we can see over time as we get out of the early status epilepticus phase, we see declines in cerebral blood flow, blood glucose and oxygen, brain tissue oxygenation, and brain glucose as the seizure activity continues. 07:38 And ultimately, that results in the potential for brain damage, We don't tend to see any risk of brain damage in the first 0 to 5 minutes, or 5 to 30 minutes. 07:47 But as we start to get beyond 60 minutes into multiple hours and days, we can see particularly with convulsive status, but also with nonconvulsive status, the potential risk of brain damage. 07:58 So again, this underscores the importance of early intervention for this medical emergency.
About the Lecture
The lecture Status Epilepticus: Stages and Pathophysiology by Roy Strowd, MD is from the course Seizures and Epilepsy.
Included Quiz Questions
Which statement is the most accurate with respect to the stages of status epilepticus (SE)?
- Stage 3 is considered refractory SE.
- Stage 1 is characterized by continuous seizure activity.
- Stage 2 is characterized by confusion without seizure activity.
- Stage 4 is characterized by continuous ictal activity on EEG.
- Stage 5 is considered super-refractory SE.
Which statement is the most accurate regarding status epilepticus? (gamma-aminobutyric acid is GABA and N-methyl-D-aspartate is NMDA)
- As the stages progress, the GABA receptors are modified.
- Stage 1 has increased GABA stimulation.
- Stage 1 has decreased NMDA stimulation.
- NMDA receptors are modified as the stages progress.
- There are no changes in either NMDA or GABA receptors.
Which statement is the most accurate with regard to the systemic impact of status epilepticus (SE)?
- If unresolved, SE can lead to cardiopulmonary collapse.
- There is an early increase of parasympathetic tone.
- Cerebral blood flow decreases initially.
- Compensatory mechanisms prevent systemic changes until stage 4.
- There is minimal impact on other organ systems throughout the SE episode.
Which statement is the most accurate with regard to brain chemistry during SE?
- Cerebral oxygen levels begin to fall after 30 minutes.
- There is an initial decrease in blood oxygen levels.
- There is an initial decrease in brain glucose levels.
- There is an initial drop in cerebral blood flow.
- Significant brain damage may occur during the first 30 minutes.
Author of lecture Status Epilepticus: Stages and Pathophysiology

Roy Strowd, MD
Customer reviews
1,0 of 5 stars
| 5 Stars |
|
0 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
2 |
2 customer reviews without text
2 user review without text
