Playlist
Show Playlist
Hide Playlist
Stable, Prinzmetal and Unstable Angina

-
Slides Ischemic Heart Disease.pdf
-
Reference List Pathology.pdf
-
Download Lecture Overview
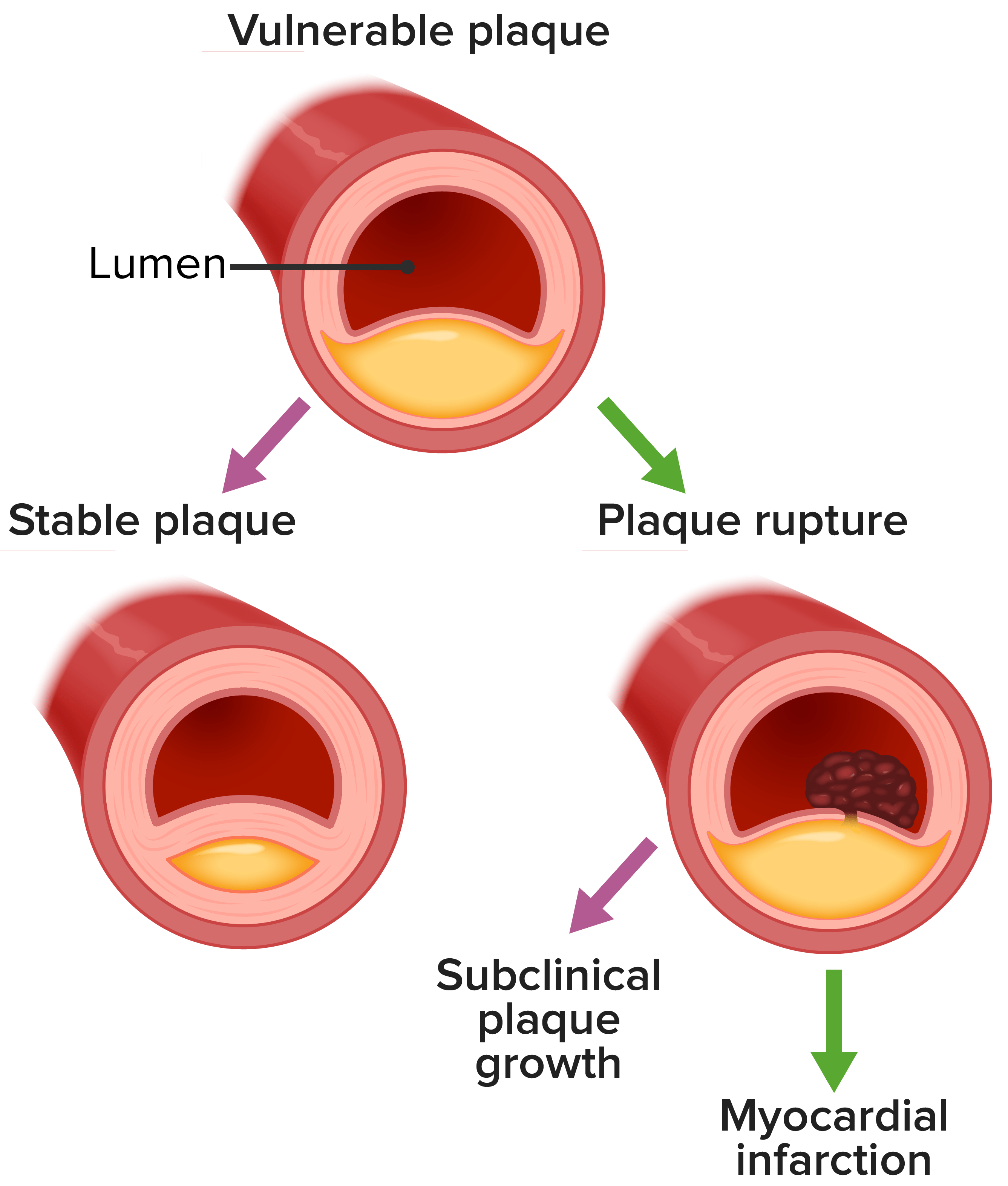
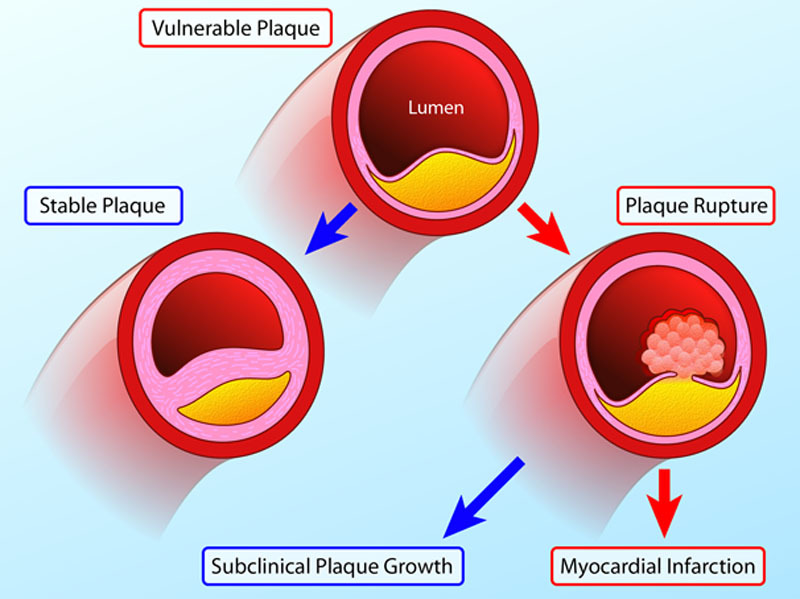
00:00 So angina pectoris, chest pain. It's an intermittent chest pain. 00:05 It's caused by transient, reversible myocardial ischemia. 00:10 So this is not a heart attack. This is the warning shot fired across the bow. 00:15 Okay. It is due to a variety of mediators that are elaborated and the primary ones can be driving angina, that chest pain sensation, is adenosine made by ischemic myocardium and it stimulates autonomic nerve fibers which sit in the pericardium and it causes the sensation of pain. 00:35 And because of the way that the viscera don't have their own independent nerves, they actually refer the pain out to certain dermatomes. 00:45 So, classically, the patient, as we'll see in a couple of slides, presents with left arm and shoulder pain, maybe left jaw pain. 00:52 Okay. So stable angina, again, means we're pretty much to the point where supply and demand are matched. 00:59 And at rest, I may have adequate supply to meet the demand. 01:03 Now if I increase my activity by running, I've increased demand and my supply may be inadequate, and I would develop, as a result of the increased pressure, the increased heartrate, the increased demand on myocardial cells to make ATP, I may tip over into the point where I get angina. 01:22 Stable means reliably, every time I run around the block once, I get chest pain. 01:28 Okay. That would be stable angina. 01:30 Alright. So stable angina presents typically because of the referred pain to the C5, C6, C7 dermatomes of the left side. 01:41 And so you get a substernal sensation that often radiates to the left arm, the left neck, the left jaw. 01:48 Some of the epigastric region or even to the back. That's classic. Okay? Patients don't always read the textbooks. 01:57 So they don't know what classic presentations they should have. 02:01 And some people's anginal equivalent, I've taken care of patients where their anginal equivalent is not anything to do with the left side. 02:08 They have right earlobe pain or they have right kind of flank pain. 02:13 So you have to take a very good history. 02:15 And just because it's right-sided pain or it's, you know, it's up here in the scalp, you need to make sure that you are not missing a slightly different anginal equivalent, okay? You have classic presentation and you have atypical presentation. 02:31 So be careful. So with stable angina, again, supply and demand is matched. 02:39 And if you have recurrent angina with relatively minimal activity, that's kind of a pain. 02:48 Literally and figuratively and metaphorically, it's a pain. 02:52 So what you can do is if you know that you want to run around the block, you know it's going to cause chest pain. 02:57 It means, you know, there is a diminished - there is an imbalance in terms of supply and demand, you can treat that by increasing coronary perfusion. 03:06 You can provide better blood supply into the tissue by giving vasodilators and the typical one is that we do a sublingual nitroglycerin. 03:15 And sublingual nitroglycerin actually is converted into nitric oxide and we already know that nitric oxide is a major smooth muscle cell relaxant which will increase the luminal diameter of the epicardial vessels. 03:28 So you can treat stable angina that way. 03:31 You probably ought to be thinking about maybe doing something much more definitive than just taking nitroglycerin but patients are adequately treated that way. 03:39 With Prinzmetal angina, this is transient coronary spasms. 03:43 Sometimes, we haven't understood ideology in terms of Catecholamines. 03:46 Other times, not so much. It's being shown here with a woman. 03:50 It's much more common in women than in men. 03:52 And it will cause a vasospasm which can give you angina. 03:57 Actually, you can have such profound vasospasm that it can actually in some cases, if it's not released, if you don't restore normal tension, normal flow to that vessel, then you can actually get a myocardial infarct. How do we treat this? Well, so they typically occur near your atherosclerotic plaques but can be in completely normal parts of the vessel. 04:20 And they respond very promptly to things like nitroglycerin or calcium channel blockers. 04:27 So those are things that you can treat and sublingual nitroglycerin is a very effective treatment for that. 04:34 And then there is angina pectoris that is associated with unstable angina due to atherosclerotic plaques. So unstable angina can be new onset chest pain. 04:47 It can be chest pain that increases with relatively lesser amounts of excertion or it can be pain at rest. 05:00 Crescendo angina is kind of the middle of those categories. 05:04 It means that, "Gee, it takes less and less and less activity for me to elicit my anginal symptoms." So it's increasingly frequent pain, progressively, less excertion. That's crescendo angina. 05:17 It's a form of unstable angina. What's going on with that? Well, it's a combination of the plaque getting bigger and bigger or intermittent little areas of plaque rupture that are not completely occlusive. 05:30 So you're not getting a myocardial infarct, but you are getting partial occlusion, and you're growing your atherosclerotic plaque by the organization of that thrombus. 05:39 So that would be a very good explanation for crescendo angina. 05:44 You can have beyond crescendo angina, now an acute plaque rupture and a complete occlusion with thrombus and that, of course, is going to give rise to a myocardial infarct.
About the Lecture
The lecture Stable, Prinzmetal and Unstable Angina by Richard Mitchell, MD, PhD is from the course Ischemic Heart Disease.
Included Quiz Questions
What is the primary mediator made by the ischemic myocardium that is responsible for the symptoms of angina?
- Adenosine
- Histamine
- Serotonin
- Prostaglandins
- Nitric oxide (NO)
Which of the following medications increases coronary perfusion and can relieve anginal symptoms?
- Nitroglycerin
- Sumatriptan
- Aspirin
- Bosentan
- Propafenone
Author of lecture Stable, Prinzmetal and Unstable Angina

Richard Mitchell, MD, PhD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
