Playlist
Show Playlist
Hide Playlist
Spinal Cord Pathology: Introduction

-
Slides 07 SpinalCordPathologies Neuropathology I.pdf
-
Download Lecture Overview
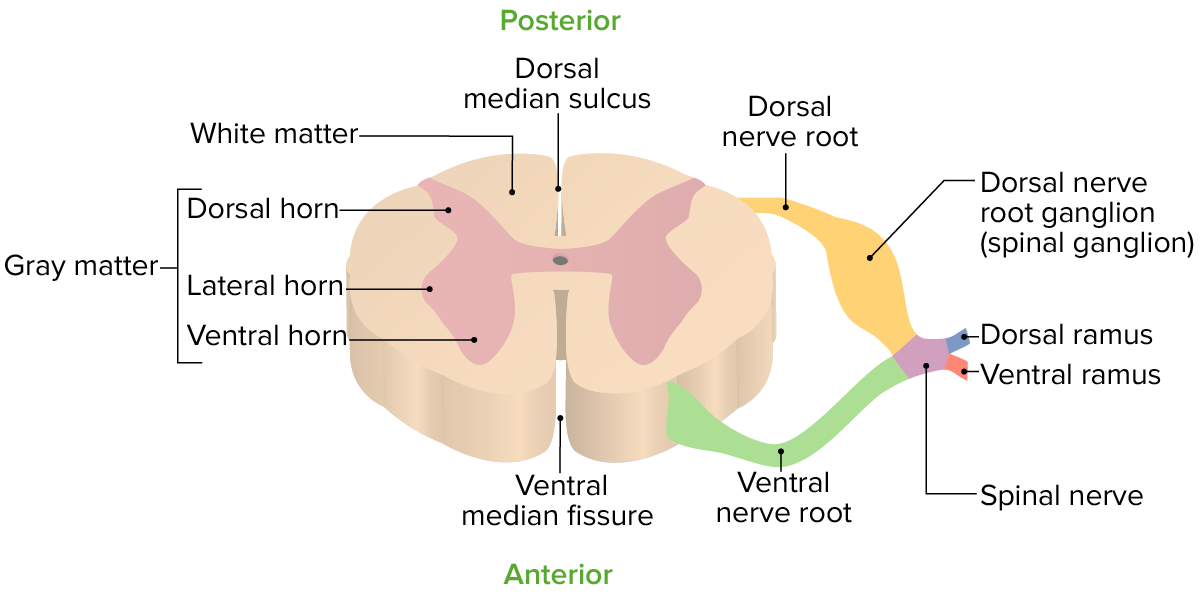
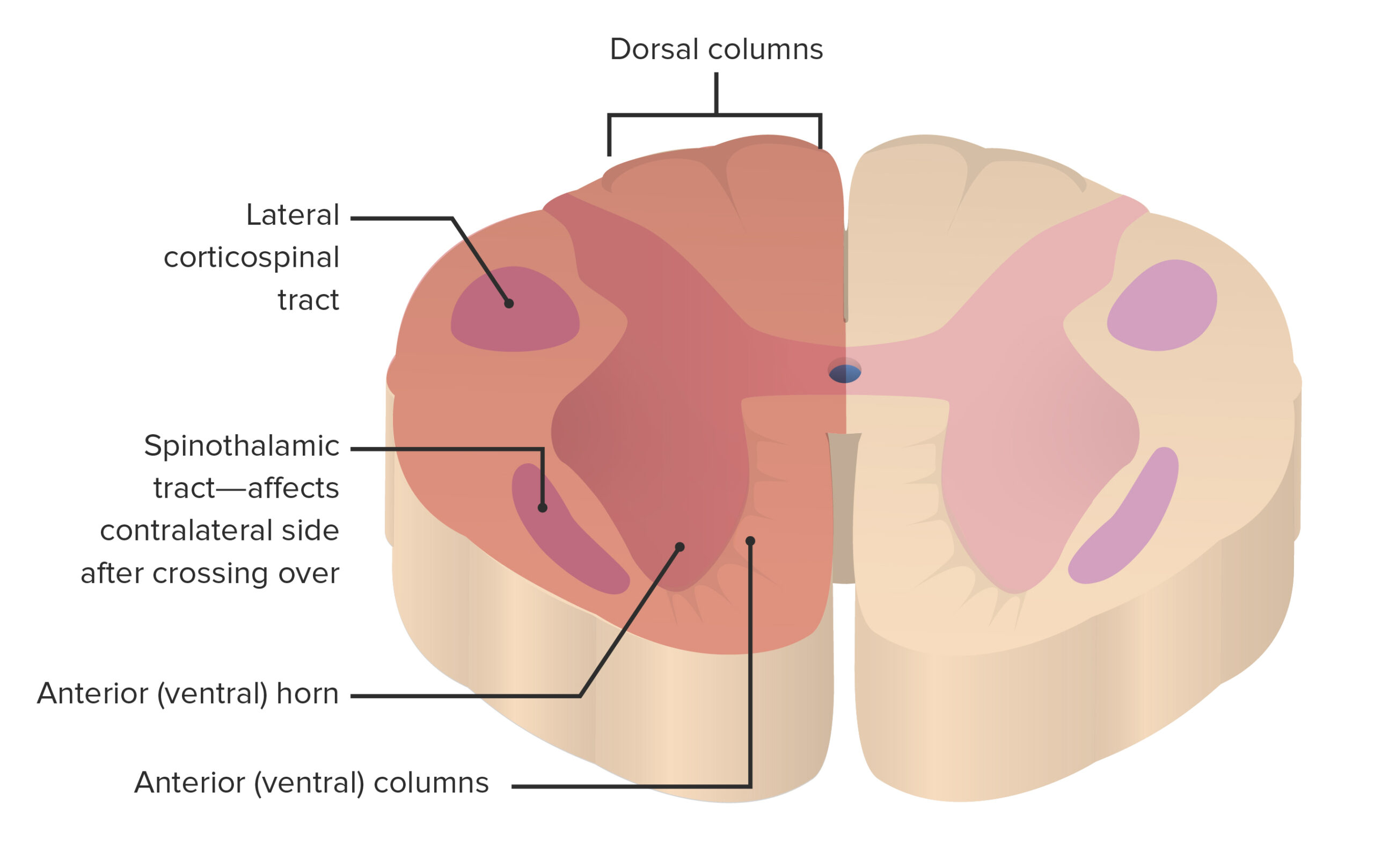
00:01 We will talk about spinal cord pathologies. 00:06 Begin by looking at some etiologies. 00:08 Trauma itself taking place resulting in spinal cord injury. 00:14 What about extraspinal mass? What if there was a metastasis that was taking place to the bone? Maybe from the breast to the vertebrae, maybe from the prostate to the vertebrae, and therefore, causing injury to the spinal cord. 00:26 Abscesses or hemorrhage even. 00:29 Extraspinal mass is therefore causing spinal cord injury. 00:32 Or intraspinal masses such as a hematoma or maybe perhaps even a tumor itself, intraspinal. 00:43 Other causes. 00:44 Inflammation referred to as being transverse myelitis, and of course, you’re quite familiar with the term myelo-. 00:54 Nutritional deficiencies such as B12 deficiency. 00:56 We’ll look at this with the megaloblastic anemia, resulting in what kind of issue? The neurologic deficit called subacute combined degeneration, right? And have ataxia due to spinocerebellar issues. 01:10 I close my eyes and have positive Romberg sign because I have damage to the dorsal column, so on and so forth. 01:17 Infection, such as tertiary syphilis may result in once again, damage to the dorsal column. 01:23 We call this tabes dorsalis. 01:25 Vascular, strokes, possibility, and AVM malformations. 01:34 What if there was a spinal cord transection? What are the signs and symptoms that you can expect? Upper motor neuron signs below the level of lesion. 01:44 What does that mean to you? Spastic paralysis and increased of reflexes, upper motor neuron below the level of the transection. 01:54 Complete sensory loss below the level because you can’t make it up, right? So therefore, you have sensory loss below the level. 02:02 Pay attention to the section and where it’s taking place. 02:07 Bowel and bladder dysfunction. 02:08 Look for incontinence. 02:11 You may see lower motor neuron signs at the level of the lesion. 02:15 Is that clear? So, at the level of the lesion, lower motor neuron, what does that mean? Flaccid paralysis. 02:22 Spastic paralysis below the level of the lesion. 02:27 In particular, hemisection of the cord is called Brown-Sequard syndrome. 02:32 Let’s take a look at the cause, such as trauma would be the most common cause. 02:37 Rarely, cord compression or partial transverse myelitis, referring to inflammation. 02:44 Most common cause, trauma. 02:47 So with the hemisection that’s taking place at the cord, what are my signs and symptoms? I’m going to walk you through this carefully and very, very deliberately. 02:57 Ipsilateral. 02:58 So think about the spinal cord where one half of it has been lesioned, ipsilateral weakness, joint position, and sensory loss. 03:07 You’ve talked about some of these with the neuroanatomy. 03:11 I just want to make sure that we’re reinforcing it here. 03:15 Contralateral, pain, and temperature loss. 03:18 Think about the spinothalamic tract and as to how it crosses over. 03:23 The center region of the spinal cord and makes its way up on the contralateral side. 03:29 So therefore, if there was a hemisection, you can expect there to be contralateral loss of pain and temperature. 03:35 And here once again, bowel and bladder dysfunction would be rare. 03:41 It could occur, but rare. 03:45 Our topic quickly here is central cord syndrome. 03:48 Where are we? In the central portion of spinal cord. 03:51 Picture that for me. 03:54 Tumor. 03:54 It would be a good idea at this point to make sure that you have a full understanding of the anatomy of the spinal cord so that we can walk through this together. 04:06 There is something called syringomyelia. 04:08 Where is my lesion right now? My topic is spinal cord pathology, specifically central cord syndrome. 04:14 With syringomyelia, what can you expect? Fluid-filled cavity within the spinal cord. 04:20 Where? Right smack dab in the middle. 04:23 Most commonly occurs in the cervical cord. 04:25 Think about where you are now, okay, because this is important. 04:29 Now, we’re going to eventually get into our signs and symptoms, and you’ve heard of cape-like issues. 04:35 What does cape-like mean? Think of Superman and he wears a cape or batman, whatever, but a cape. 04:41 And where does the cape then drape you? Oh yes, over the shoulders, right? The cervical region. 04:47 And we’ll talk about cape-like lesions in a second, but understand as to what that means. 04:51 Don’t just memorize cape. 04:53 That makes no sense. 04:54 That will tell you where lesion is taking place. 04:58 It can occur after trauma. 05:00 It can occur in conjunction with Chiari malformation. 05:06 Chiari, what does that mean? Arnold-Chiari. 05:08 Not Budd. 05:10 Are we okay here? Budd-Chiari, uh-uh, has nothing to do with the spinal cord, huh? It has nothing to do with CNS pathology. 05:20 Budd-Chiari was hepatic vein thrombosis. 05:23 Keep that separate. 05:24 Syringomyelia can occur in conjunction with a Chiari malformation. 05:28 It generally spares the dorsal columns, but these can be affected by B12 deficiency or tertiary syphilis. 05:34 A Chiari malformation is a congenital condition causing abnormalities of the brain at the junction of the skull with the spine. 05:40 Chiari one malformation means low-lying cerebellar tonsils without other congenital brain malformations, downwardly-displaced in the foramen magnum. 05:49 Some patients are asymptomatic, but some have syringomyelia symptoms. 05:54 These are lower motor neuron signs in the upper extremities, causing loss of pain and temperature sensation of the upper torso and arms in a cape-like distribution, loss of muscle strength in the hands and arms, aswell as hypotonia can also be expected. 06:07 In the legs, there may be upper motor neuron signs including spasticity, positive Babinski sign, and loss of function or reflexes. 06:15 Chiari two malformation is also named “Arnold-Chiari” where the cerebellar tonsils and medulla go through the foramen magnum into the upper cervical canal, and occurs almost exclusively in patients with myelomeningocele. 06:28 These patients may have symptoms of syringomyelia as well as other symptoms.
About the Lecture
The lecture Spinal Cord Pathology: Introduction by Carlo Raj, MD is from the course Spinal Cord Pathology. It contains the following chapters:
- Spinal Cord Pathologies
- Spinal Cord Transection: Symptoms
- Brown-Sequard Syndrome
- Central Cord Syndrome
Included Quiz Questions
What is the name and site of the typical lesion in the spinal cord caused by vitamin B12 deficiency?
- Subacute combined degeneration (SCD) in the dorsal columns
- Subacute combined degeneration (SCD) in the ventral columns
- Subacute combined degeneration (SCD) in the anterior gray horns
- Subacute combined degeneration (SCD) in the olivary nuclei
- Subacute combined degeneration (SCD) in the transverse columns
A combination of upper motor neuron signs in the lower extremities and lower motor neuron signs in the upper extremities is caused by which type of lesion?
- Central cord syndrome (syringomyelia)
- Budd-Chiari syndrome
- Anterior spinal cord syndrome
- Posterior spinal cord syndrome
- Tabes dorsalis
A young man with a history of Chiari malformation presents to the ED with weakness in his extremities. Which of the following is the most likely finding on physical examination?
- Loss of pain and temperature sensation in a cape-like distribution
- Loss of pain and temperature in the lower extremities
- Loss of pain and temperature in the upper extremities
- Lower motor neuron signs in the lower extremities
- Upper motor neuron signs in the upper extremities
Author of lecture Spinal Cord Pathology: Introduction

Carlo Raj, MD
Customer reviews
2,0 of 5 stars
| 5 Stars |
|
0 |
| 4 Stars |
|
1 |
| 3 Stars |
|
0 |
| 2 Stars |
|
1 |
| 1 Star |
|
2 |
Understanding that it is an introduction, so I would not expect a lot of details, assuming that there will be other videos that go more in depth. I like the update provided a little more information on Arnold Chiari than other lectures. I would have liked some animation to help illustrate.
I understand the point of an "introductory" lecture, but this is well below subpar. I needed detailed explanations of the various types of Spinal Cord injuries. I looked at the other video in the "series", but this is well below that of what I expect from a clinical neurology section.
I don't want to sound unkind, but this is not good. Not enough exact facts and description of the conditions, too many unnecessary phrases that don't help me connect with Dr. Raj and what he is trying to teach me. This was a waste of my precious time.
Im sorry Dr Raj, I really enjoyed your cardiology series, but the neurology is subpar to put it politely. zero detail, just a bunch of bullet points and basic stuff a first year pre-med student already knows. no detail as to the pathophysiology, treatment or any of that. If I have to go back to biochem or neuroanatomy for all that then what's the point of this series?
