Playlist
Show Playlist
Hide Playlist
Sarcoidosis: Extrapulmonary Manifestations


-
Slides 06 ILD InterstitialLungDisease RespiratoryAdvanced.pdf
-
Download Lecture Overview
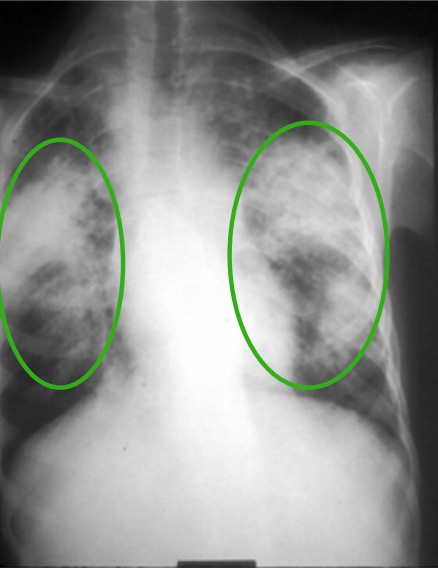
00:00 So the manifestation of extrapulmonary sarcoid are complicated because there merely are different types. The common forms are eye involvement with an acute uveitis and scleritis. Parotid and salivary gland enlargement which can lead to palpable masses, now normally, this is symmetrical and the patient may get dry mouth in sicca syndrome. 00:24 A neurological involvement is not uncommon and is quite a serious problem because it may lead to peripheral neuropathy, cranial nerve palsies, and deposits in the central nervous system into chronic neurological defects. Skin involvement is also common. Now, the acute presentation as we discussed is with painful lumps on the shin, erythema nodosum. But the chronic form is quite different. It's a non-tender blue nodules especially in scars doesn’t have to be in the lower legs, it could be anywhere in the body, and that forms a powerful infiltration in patients with chronic sarcoidosis. And important diseases are cardiac disease because that can lead to conduction defects and it actually present with disrythmias including sudden death. And in some patients, also can lead to restrictive cardiomyopathy. So that’s a very important form of sarcoid that’s not uncommon but not the commonest presentation. 01:21 And nasal destruction is a very rare form of sarcoid which leads to very unpleasant destruction of the nose. As well as those conditions, you can also have sarcoid affecting the reticuloendothelial system causing a hepatosplenomegaly and abnormal liver function test but not normally causing any functional liver impairment that is clinically detectable. The spleen is frequently enlarged due to infiltration with sarcoidosis, and you may get nodal disease in the extrathoracic lymph nodes that could be in the neck, in the abdomen, in the groin. 01:56 Joints are often involved to a certain extent with arthralgia, and you can get bone system in the infiltration of sarcoidosis … around the joints. And endocrine problems are a potential issue. They’re relatively rare but they’re important because they require treatment. 02:13 For example, a hypercalcaemia can occur in 5% of patients with chronic sarcoidosis and will need treatment. Occasionally, you get infiltration in the pituitary area with sarcoid granulomas leading to hypopituitarism and diabetes insipidus. Very rare but very important manifestation of the disease. So, how do we investigate patient with sarcoidosis? It is similar to other interstitial lung disease with the chest X-ray, lung function, and a CT scan. Unfortunately, these normally add upto the picture which is very suggestive with sarcoidosis, for example, if the chest X-ray will show bilateral, hilar, and mediastinal lymph node involvement and upper lobe infiltrations as we have already discussed. 02:56 The lung function will show restrictive obstructive picture with a fall in transfer factor, a little seen as your hypersensitivity pneumonitis where you get a mixed restrictive obstructive picture rather than the pure restrictive picture. And the CT scan will show bilateral, hilar, and mediastinal lymph node enlargements, diffused parenchymal nodules with the upper lobe predominance we’ve already discussed, and actually, very characteristically you often see little nodules forming on the edge of the pleura or on the oblique and horizontal fissures. 03:29 These appearances would very strongly suggest the diagnosis of sarcoidosis. A bronchoscopy may show a lymphositosis in the lavage, and blood tests are important because you need to exclude the presence of the endocrine abnormalities where we discussed hypercalcaemia, for example, to look for liver involvement by doing little function tests. And also, the serum angiotensin converting enzyme (ACE) level is often raised in patients with sarcoidosis. Now, it's actually not particularly a good test because it is often raised in conditions where there is no sarcoidosis. 04:06 However, in a patient with sarcoid and a raised serum ACE level, it can be useful to monitoring disease progression. For example, as the disease gets better, then the serum ACE level would fall. But if the disease is not improving, then the serum ACE level will remain high. 04:23 Now, the test for involvement with other organs is dictated by the clinical presentation of the patient. So if you suspect there might be cardiac disease, you need to do an ECG, an echocardiogram. If you suspect there might be a mediastinal involvement, you have to do abnormal ultrasound and CT scans and look for enlarged liver, enlarged spleen, and enlarged abdominal nodes. And then neurological involvement requires CT scans, MRI of the brain, etc etc. 04:48 So the extrapulmonary sarcoidosis may require a very large range of different tests depending on what the presentation of the patient might be.
About the Lecture
The lecture Sarcoidosis: Extrapulmonary Manifestations by Jeremy Brown, PhD, MRCP(UK), MBBS is from the course Interstitial Lung Disease (ILD).
Included Quiz Questions
Which of the following is associated with extrapulmonary sarcoidosis?
- Lupus pernio
- Lupus erythematosus
- Lupus profundus
- Lupus miliaris disseminatus faciei
- Lupus vulgaris
Which cardiac manifestation can a patient with sarcoidosis present with?
- Restrictive cardiomyopathy
- Hypertrophic obstructive cardiomyopathy
- Dilated cardiomyopathy
- Cardiac vegetations
- Mitral valve prolapse
Which of the following metabolic changes are associated with sarcoidosis?
- Hypercalcemia
- Hypocalcemia
- Hyponatremia
- Hyperkalemia
- Hypokalemia
Which of the following diseases are associated with extrapulmonary sarcoidosis?
- Diabetes insipidus
- Syndrome of inappropriate secretion of antidiuretic hormone (SIADH)
- Hyperthyroidism
- Hypoparathyroidism
- Diabetes mellitus
Which of the following serum enzymes may increase in patients with sarcoidosis?
- Angiotensin converting enzyme
- Cholecystokinin
- Pepsinogen
- Serotonin
- Brain natriuretic peptide
Author of lecture Sarcoidosis: Extrapulmonary Manifestations

Jeremy Brown, PhD, MRCP(UK), MBBS
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
