Playlist
Show Playlist
Hide Playlist
Sarcoidosis


-
Slides 06 ILD InterstitialLungDisease RespiratoryAdvanced.pdf
-
Download Lecture Overview
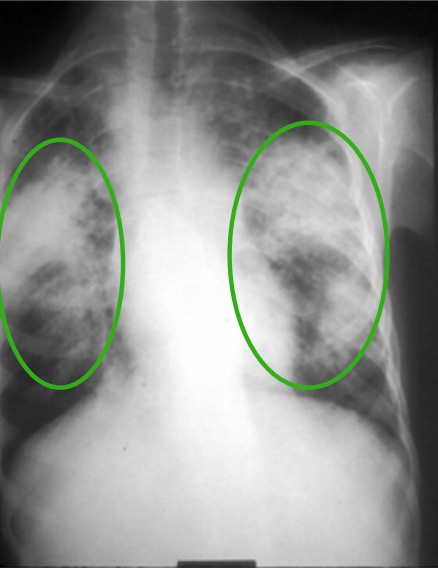
00:01 The subject of this talk is a specific form of interstitial lung disease called sarcoidosis. 00:05 Now, this disease, you get infiltration of the lung and extrapulmonary tissue with non-caseating granulomas. This seems to be a cell mediated reaction, but the reason for that, why it happens remains unknown and is probably different depending on the patient. The thing about sarcoidosis, a light tuberculosis and lung cancer, it's one of the three lung diseases that can have multisystem presentation, because not only does it affect the lung, but it affects many extrapulmonary sites. As seen in this diagram, some of the common examples are the eyes and the skin, your neurological system, lymph nodes, cardiac, joint, liver, and spleen, etc. This means that sarcoid, when it's chronic, can be very variable in its presentation depending on the pattern of disease of which organs have been affected by the disease. 00:58 Importantly, the diagnosis can be made and needs to be confirmed by a biopsy to show these non-caseating granulomas which are very distinctive for the sarcoidosis. 01:09 Clinical presentation of sarcoid, well the average age of presentation is a young adult, between 20 and 40. It is probably slightly more common in women than it is in men. 01:21 It is actually very common in the Afro-Caribbean populations for reasons which are not clear. 01:25 But still, it is very significantly present in the Caucasians as well. There are acute presentations and there are chronic presentations of sarcoidosis. Acute presentations tend to be relatively similar. The patient will be a young adult. They will present with bilateral hilar lymphadenopathy which are enlarged lymph nodes visible in a chest X-ray in the middle of the chest. And they may have erythema nodosum which is a skin rash which affects the lower parts of the leg on the anterior shin when they will get raised tender lumps which are one or two centimeters across, and very clinically obvious and very easy to diagnose as erythema nodosum. 02:03 The patient will feel a bit unwell, they may have a bit of a temperature, a bit of sweat, a bit of arthralgia, pains in their joints, and may be feeling just a bit miserable under the weather. This disease, this acute syndrome is often called Lofgrens syndrome and only lasts for a few weeks or months and most patients will resolve spontaneously with no recurrence to the sarcoid thereafter. And treatment is often not required. 02:28 Chronic presentation is different. The patient will present an insidious disease. It comes on slowly. It can be progressive over time. It can be stable over time. It can have inflares, it can have periods where it gets best and gets worse, waxes and wanes. And the presentation really depends in which organs are affected, and that is why chronic sarcoidosis can be very varied in this presentation because it depends on which particular organs are involved in that specific patient. So, if we’are talking about pulmonary sarcoidosis, lung involvement, the common presentations with acute sarcoidosis is bilateral hilar lymphadenopathy, enlarged lymph nodes, visible on a chest X-ray and a CT scan. These lymph nodes tend to be symmetrical and smooth, even in distribution on both sides. And they don’t really tend to cause too much in the way since they can cause a cough. The differential diagnosis for enlarged lymph nodes in the chest is tuberculosis, lymphoma and cancer. So serious diseases, but all of those diseases tend to cause non-symmetrical enlargement of the lymph nodes. And in many patients with acute sarcoid, the combination of symmetrical lymph nodes and erythema nodosum is adequate in itself to be happy that they have acute sarcoidosis rather than any of these other more complicated diseases. As well as the lymph nodes, patients with chronic disease may also develop infiltrates in the lung, and these are normally a reticulonodular infiltrations in both upper lobes. This leads to volume loss, and often, you can actually hear when you listen to the lungs any crepitations over these. And the patient can be surprisingly asymptomatic with quite a dramatic chest X-ray. But eventually, this sort of disease will cause dyspnoea due to lung loss and restrictive lung function problems. Occasionally, you get end-stage sarcoidosis which looks very much like the UIP form of pulmonary fibrosis as we discussed in the earlier lecture. And some of these infiltrates coalesce to form nodules in the lung which are much more larger than just the micronodular infiltrate you might normally get. Very occasionally, you get patients with ground glass infiltrates, and thats one of the presentations that are more severe acute disease than normal. So this is an example of a chest X-ray and you can see in both upper lobes, there is a sort of interstitial infiltration and there is distortion of the hilar and loss of volume. And in some patients there is a bit of coalesce lung infiltration where you get more lump-like material present. And that is just the areas where there is actually quite extensive sarcoidosis. You can stage pulmonary sarcoidosis, and this is the scheme that’s used for stages not to four, not having no pulmonary disease, just extrapulmonary disease only, one being the classic acute bilateral hilar lymphadenopathy, BHL presentation, which is unlikely to progress with 90% of patients for admission. Or you can have the bilateral hilar lymphadenopathy presenting with some parenchymal infiltrations, and these patients are probably a little bit more likely to progress than just the ones with the lymph nodes alone. And then there's the more chronic forms. We have parenchymal infiltrations which can go into remission but normally do not, and in fact, can be progressive over time and eventually to advanced pulmonary fibrosis stage four disease with marked dyspnea and restrictive failure.
About the Lecture
The lecture Sarcoidosis by Jeremy Brown, PhD, MRCP(UK), MBBS is from the course Interstitial Lung Disease (ILD).
Included Quiz Questions
Which hypersensitivity reaction is associated with sarcoidosis?
- Type 4
- Type 1
- Type 2
- Type 3
- Sarcoidosis is not associated with hypersensitivity reactions.
Which dermatological condition is associated with sarcoidosis?
- Erythema nodosum
- Erythema marginatum
- Erythema larva migrans
- Erythema toxicum
- Erythema multiforme
A patient presents with a cutaneous finding consistent with erythema nodosum. The patient also has large symmetrical hilar lymphadenopathy. Which of the following is the patient's most likely diagnosis?
- Sarcoidosis
- Tuberculosis
- Lymphoma
- Cancer metastasis
- Pneumonia
Which of the following clinical presentations is NOT characteristic of patients with sarcoidosis?
- Pulmonary consolidation
- Reticulonodular infiltrates on lung X-ray
- End-stage fibrosis on lung CT
- Medium-sized nodules on lung X-ray
- Ground-glass appearance of lung tissue on X-ray
Which of the following stages of pulmonary sarcoidosis is found in a patient with bilateral hilar lymphadenopathy and parenchymal infiltrate?
- Stage 2
- Stage 3
- Stage 4
- Stage 5
- Stage 1
Author of lecture Sarcoidosis

Jeremy Brown, PhD, MRCP(UK), MBBS
Customer reviews
3,0 of 5 stars
| 5 Stars |
|
0 |
| 4 Stars |
|
0 |
| 3 Stars |
|
1 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Content good but delivery too fast and monotonous, with little or no emphasis on the really essential parts. Overall result is a boring lecture unfortunately.
