Playlist
Show Playlist
Hide Playlist
Rib Cage Region: Introduction

-
01 Slides Cymet Rib Cage Region General Principles.pdf
-
Reference List Osteopathic Manipulative Medicine.pdf
-
Download Lecture Overview
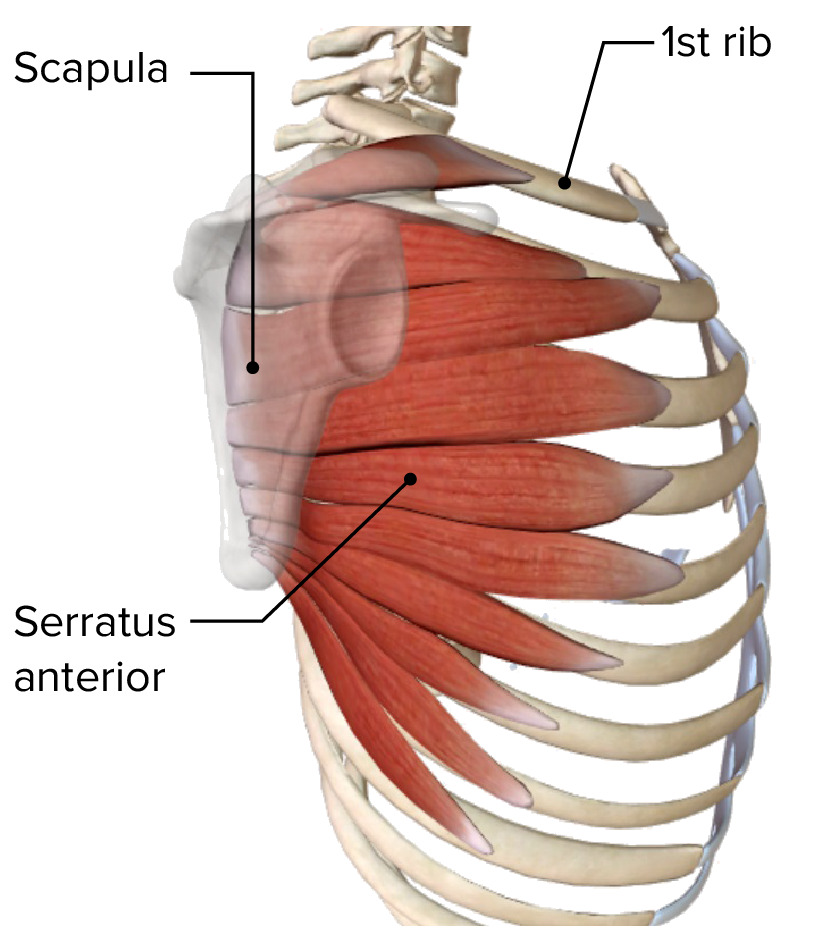
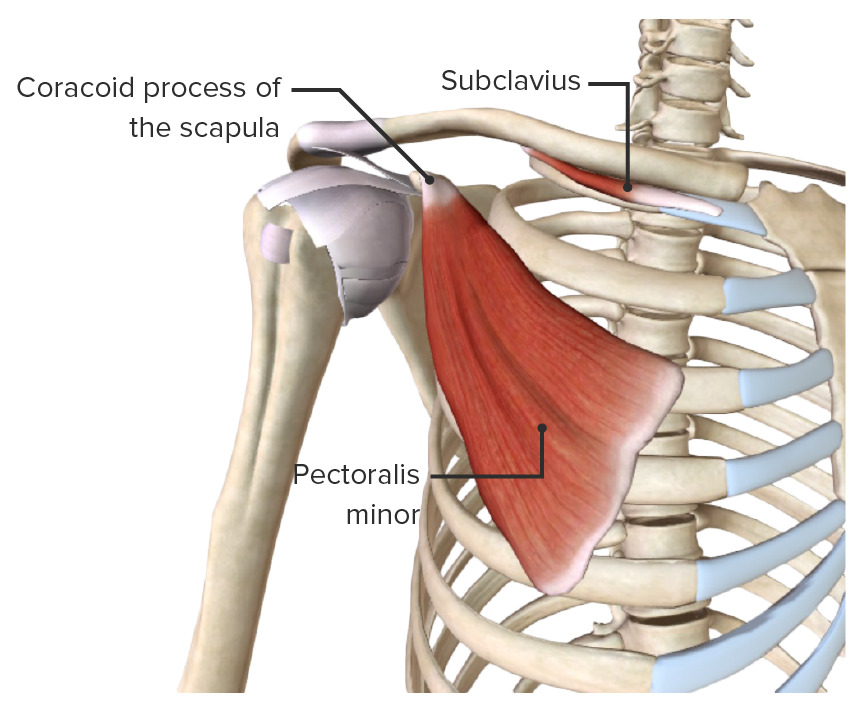
00:00 The ribs are regional organs that control mineral deposition, mineral regulation, as well as having structure and functional relationships. In osteopathic medicine, I want to focus on the structure and function of the ribs so we can talk about their importance in body motion and body functioning. 00:19 If you look at the rib cage, it’s a collection of ribs encasing the chest wall cavity. It's encasing the heart and the lungs. It's encasing a number of arteries,veins as well as other structures within the thorax. So, the ribs, which start of small and get bigger as you go down, are elastic arches of bone. They are flat, they are thin and they start in the back. They come down and then back up, not as high as they started, by the manubrium and the sternum. They fused together in the front and that forms the rib cage that encompasses and holds the thoracic organs. So, the chest is an IKEA-like creation that creates the chest cage and protects the heart, lungs and major vessels. 01:09 When you look at the individual ribs, again they are curved and somewhat sickle-like and they twist along a longitudinal access, so it’s going to be attached in the back to the spine and then from the spine to the transverse process come down and then up, not as high as it started, but it will fuse in the front to form the rib cage. The true ribs, ribs 1 through 7, are the ribs that will fuse in the front and become part of the costal cartilages. The false ribs are 8 through 12 because their cartilages are joined to that of the rib below or above it, it’s an indirect connection. Ribs 1 through 7 are true ribs. They attach directly to the sternum and have their own costal cartilage for each rib. The vertebrochondral ribs, ribs 8 through 10, attach in the front through other ribs. 02:11 The floating ribs 11 and 12 have different motion, they’re not part of the rib cage but they do have muscle attachments and affect the motion of the ribs. So if you look at the chest cavity again, you can notice that there are places like the jugular notch or vessels and organs will enter the chest cavity. You’ve got the sternum and manubrium, which is the connection point for the ribs and then you have the clavicle coming back to the scapula forming a strut. So there are a lot of connections and articulations here that matter. So, we’re going to focus on the back and the connections because it's important to get a good understanding of how the ribs are functioning and where they sit anatomically. So when you look at the rib, it’s going to have a number of connections on the rib itself. The first one attaching to the spine and the second one attaching to the transverse process of the spine above it and this is going to stabilize it and allow motion. 03:13 So posteriorly, the articulations for the typical ribs are the costovertebral and the costotransverse junctions. That’s where it's connecting. When you go anteriorly, you will see that the costochondral junction, the bone and the cartilage are going to transition between osseous ribs and cartilage. 03:34 There's a connector, another point, that brings the bone to the manubrium so that motion is easier. 03:41 There is more motion when you have cartilage than when you have bone. And these things are going to change over time and over your life. So the ribs get larger from rib 1 to rib 10. They expand in size, they expand in angle and they change in how their motion is going to be occurring. This also changes throughout age and we know that the ribs do start to fuse more after 18 years of age in men, 21 years of age in women. By 30 years of age, the cartilage and the bone are more fused and more consistent into the pattern they’re going to be for life. So we do see some change and this is different for each of the ribs, the longer or larger ribs are going to solidify and fuse later. The floating ribs act differently, that’s the 11th and 12th ribs that are posteriorly they’re going to have abdominal muscle and core muscle attachments that are going to affect breathing, affect motion and have a different flexibility than the other ribs. As a physician, most of the time we’re focusing on the ribs it’s after a car accident or after trauma when the rib cage gets injured, it's somewhat delicate and sensitive to trauma. So it’s something that whenever you see a car accident victim you do need to be checking and looking for. Another area where we focus a lot on the ribs in osteopathic medicine is the 1st rib in the thoracic outlet, thoracic inlet, thoracic aperture, same thing. The hole on the top, the top of the rib cage is going to be the thoracic outlet, it’s going to be the thoracic inlet, different names for the same area. And the thoracic aperture is the opening that has a lot of the vessels going through. You’ve got the brachial plexus, you’ve got the subclavian artery and vein going just above the rib and under the clavicle and you’re going to have muscle and ligament attachments that matter. So this is a key area because oftentimes you’ll have nerve impingement, you’ll have arterial impingement or you have to find the artery or vein there, so these matter. There is also a lot of lymphatic drainage that can be a site of congestion or change and we often examine the apex of the lung and the mediastinum here and listen at this point to make sure you’ve got good transmission of sound and airflow.
About the Lecture
The lecture Rib Cage Region: Introduction by Tyler Cymet, DO, FACOFP is from the course Osteopathic Diagnosis of the Ribs. It contains the following chapters:
- Rib Cage Region
- Ribs 1–10
Included Quiz Questions
What is the group of ribs that is directly attached to the sternum?
- True ribs
- False ribs
- Vertebral ribs
- Vertebrochondral ribs
- Floating ribs
Which ribs have no anterior attachments to the sternum?
- Ribs 11 and 12
- Ribs 1 to 3
- Ribs 6 to 8
- Ribs 8 and 9
- Ribs 4 to 9
What is the anterior transition area between the osseous rib and the cartilage of the rib?
- Costochondral junction
- Costovertebral junction
- Costotransverse junction
- Sternal angle
- Manubrium
Which rib is found at the area of the thoracic inlet?
- Rib 1
- Rib 2
- Rib 3
- Rib 11
- Rib 12
Author of lecture Rib Cage Region: Introduction

Tyler Cymet, DO, FACOFP
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
