Playlist
Show Playlist
Hide Playlist
Review: Shoulder Pathology and Anatomy

-
Slides Shoulder pain.pdf
-
Reference List Rheumatology.pdf
-
Download Lecture Overview
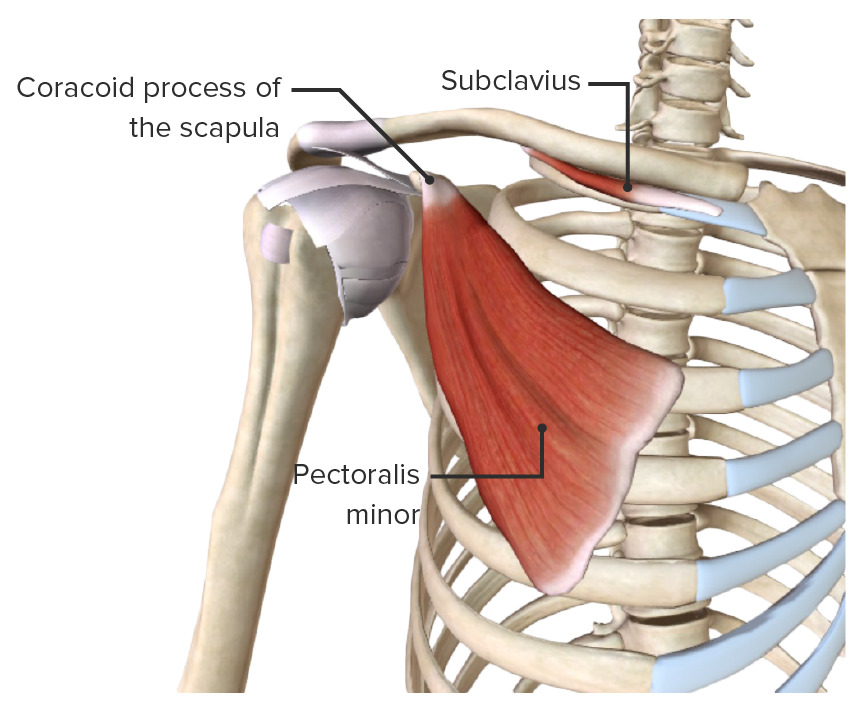
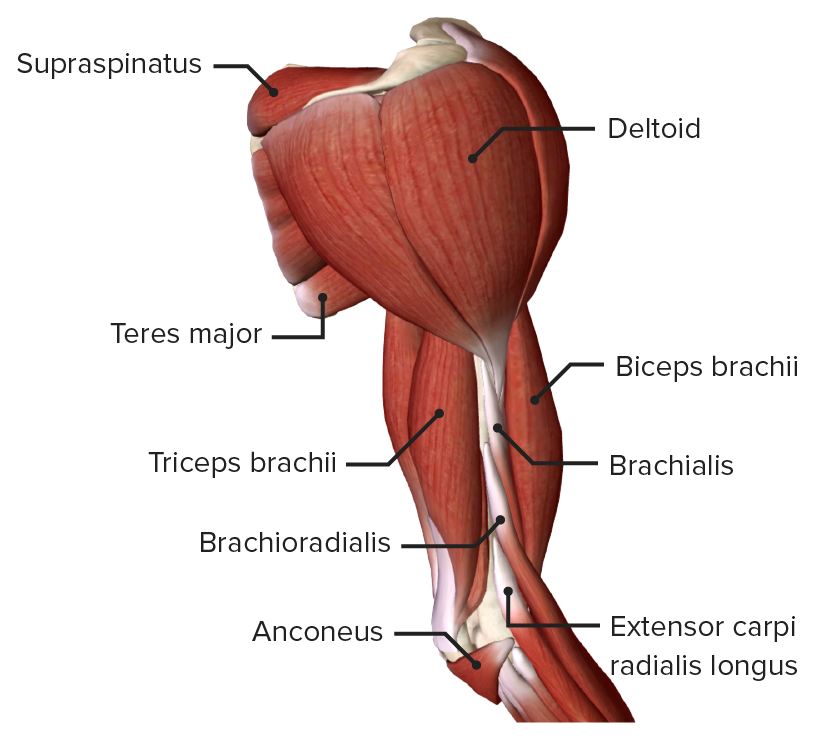
00:00 We like to break up the differential diagnoses of shoulder pain based on anatomical location. 00:07 First up, capsular disease. The 2 major types of disease of the capsule are adhesive capsulitis and glenohumeral arthritis of the glenohumeral joint. Adhesive capsulitis is essentially a progressive stricture of the capsule itself around the glenohumeral joint. Next up is rotator cuff disease, rotator cuff tendinosis or impingement which can progress to involve a rotator cuff tear. Oftentimes there is concomitant subacromial or subdeltoid bursitis at the same time. And then we have biceps disease, which itself doesn't involve the joint but it is an associated peri-articular structure. So biceps tendonitis or potentially a biceps tendon tear or rupture. 00:50 And last up, a category we're not going to focus on much today are a variety of inflammatory infectious causes of shoulder pain. Generally speaking, in the absence of any suggestion of systemic involvement like fevers or chills or other affected organ systems, we can pretty much take this category off the list. That still though leaves off a lot of possibilities above. So, let's review our anatomy just a little bit more. Alright, so now we have a picture, a cross-section of the shoulder itself. And the first thing I want us to hone in on is the glenohumeral joint. Now keep in mind, the glenohumeral joint is a ball and socket type joint that is actually fairly unstable, if not for the rotator cuff and the glenoid labrum which provides some additional structure instability to an otherwise very loose joint. When we talk about capsular causes of pain, we're talking about either arthritis at the glenohumeral sulcus or we're talking about disease of the glenoid capsule or we're talking about adhesive capsulitis. The next structure we want to focus on is the rotator cuff and specifically the supraspinatus tendon which is shown here on the right. 01:57 The rotator cuff is not really responsible for the strength of shoulder movement. That would really be more of the latissimus dorsi muscles and the deltoid muscles. The rotator cuff instead is responsible for stabilizing the head of the humerus in the glenoid fossa. Above the rotator cuff is the subacromial bursa. Now actually the subacromial bursa and the subdeltoid bursa are the same structure, we're just talking about different areas of that structure whether it's underneath the deltoid which is further lateral or more proximal would be underneath the acromial head. The subacromial bursa in any situation where there is significant rotator cuff disease or tendinopathy, you're probably going to see some inflammation in that bursa and as you can see the picture that bursa is essentially designed to buffer the rotator cuff which lies right between 2 bones, the acromion and the humeral head. And lastly, another important structure is the biceps tendon specifically the long head of the biceps tendon and that is also shown here in the picture on the right. The long head of the biceps tendon is inserting into the glenoid labrum right where the glenohumeral joint occurs and if there's any problem with the biceps tendon a a person is certainly going to experience pain in the shoulder and it will be difficult to tease a part whether the disease is the tendon of the long head of the biceps tendon or if it's rotator cuff pathology or something else going on with the glenoid capsule. Alright, so with that overview let's look back at our case. What we're seeing here right off the bat when we look at range of motion is that he is having significant reductions in range of motion both actively and passively with abduction and external rotation. Now, we should probably take another step back and remind ourselves what those movements mean when we're talking about the shoulder. So as I said, the shoulder is a ball and socket joint which actually makes it kind of complicated because it has 3 degrees of freedom. So we have to make sure we use the right language to describe how we're moving the shoulder around. So, first up is flexion and that simply means moving the arm in front of your body. In contrast, extension is moving the arm directly behind you. Next up is abduction and that's going to be moving the arm out to the side compared with adduction which is moving the arm across your body. In addition and not pictured here is internal and external rotation starting with your arm in front of your body with an elbow at 90 degrees, you're moving your arm out for external rotation and in for internal rotation. So, revisiting our patient story, he was having limited active and passive range of motion with abduction so he is only able to get his arm to about 90 degrees and external rotation was quite limited at only 30 degrees. In addition, he is reporting pain and weakness with external rotation. So what is it that allows somebody to move their arm in external rotation? What are the muscles and structures involved?
About the Lecture
The lecture Review: Shoulder Pathology and Anatomy by Stephen Holt, MD, MS is from the course General Approach to Arthritis and Joint Pain.
Included Quiz Questions
The glenohumeral joint is a(n)…?
- ...ball-and-socket joint.
- ...hinge joint.
- ...pivot joint.
- ...ellipsoidal joint.
- ...saddle joint.
The long head of the biceps originates from the...?
- ...glenoid labrum.
- ...acromion.
- ...coracoid process.
- ...humeral greater tuberosity.
- ...humeral lesser tuberosity.
Author of lecture Review: Shoulder Pathology and Anatomy

Stephen Holt, MD, MS
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
THE WAY HE TEACHES MAKES TOPIC EASE AND HE ALWAYS GOES STEP BY STEP HE KNOWS WHERE TO STRESS THINGS JUST LOVED THE LECTURES
