Playlist
Show Playlist
Hide Playlist
Review of the Vestibular System and Evaluation of Vertigo

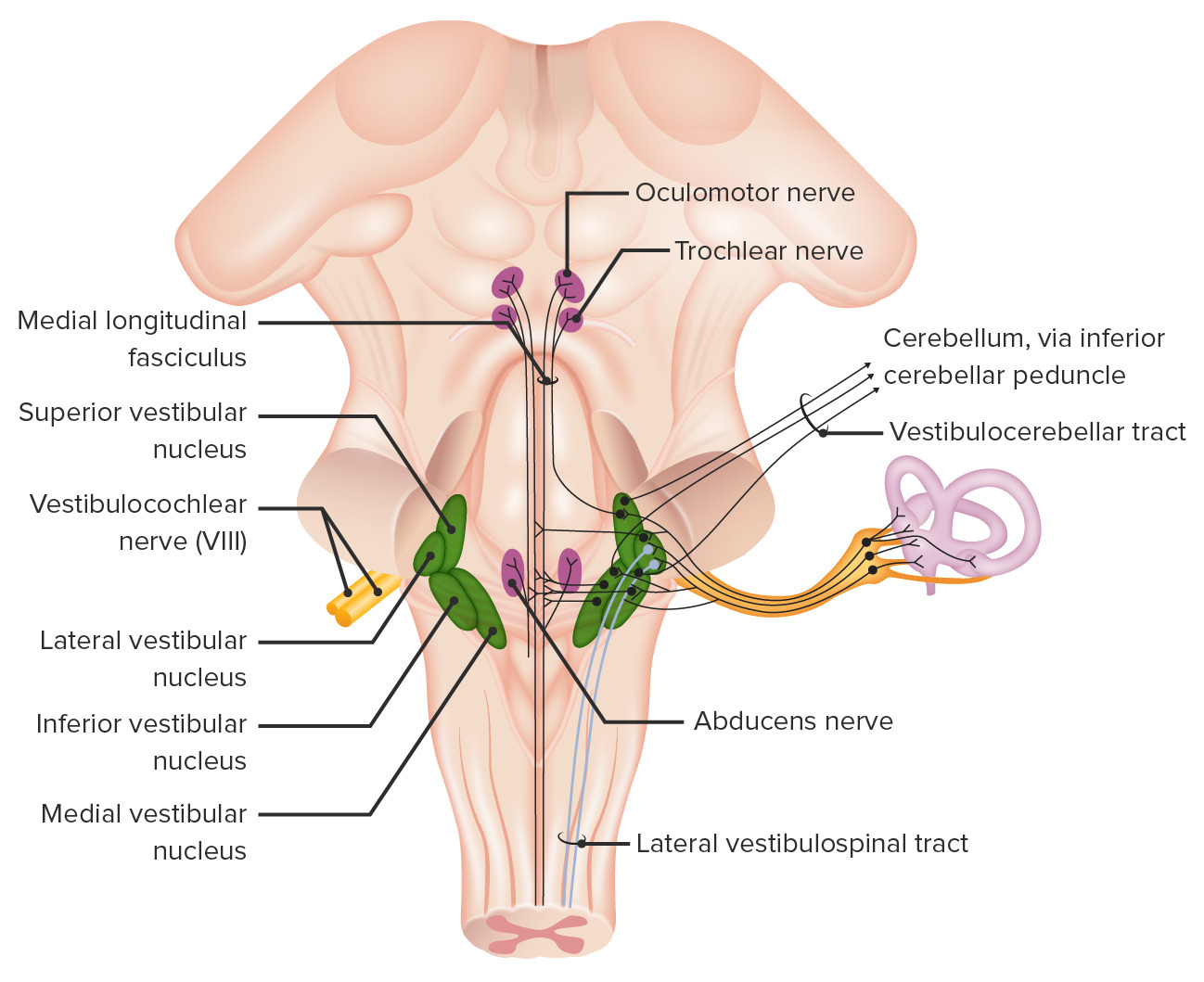
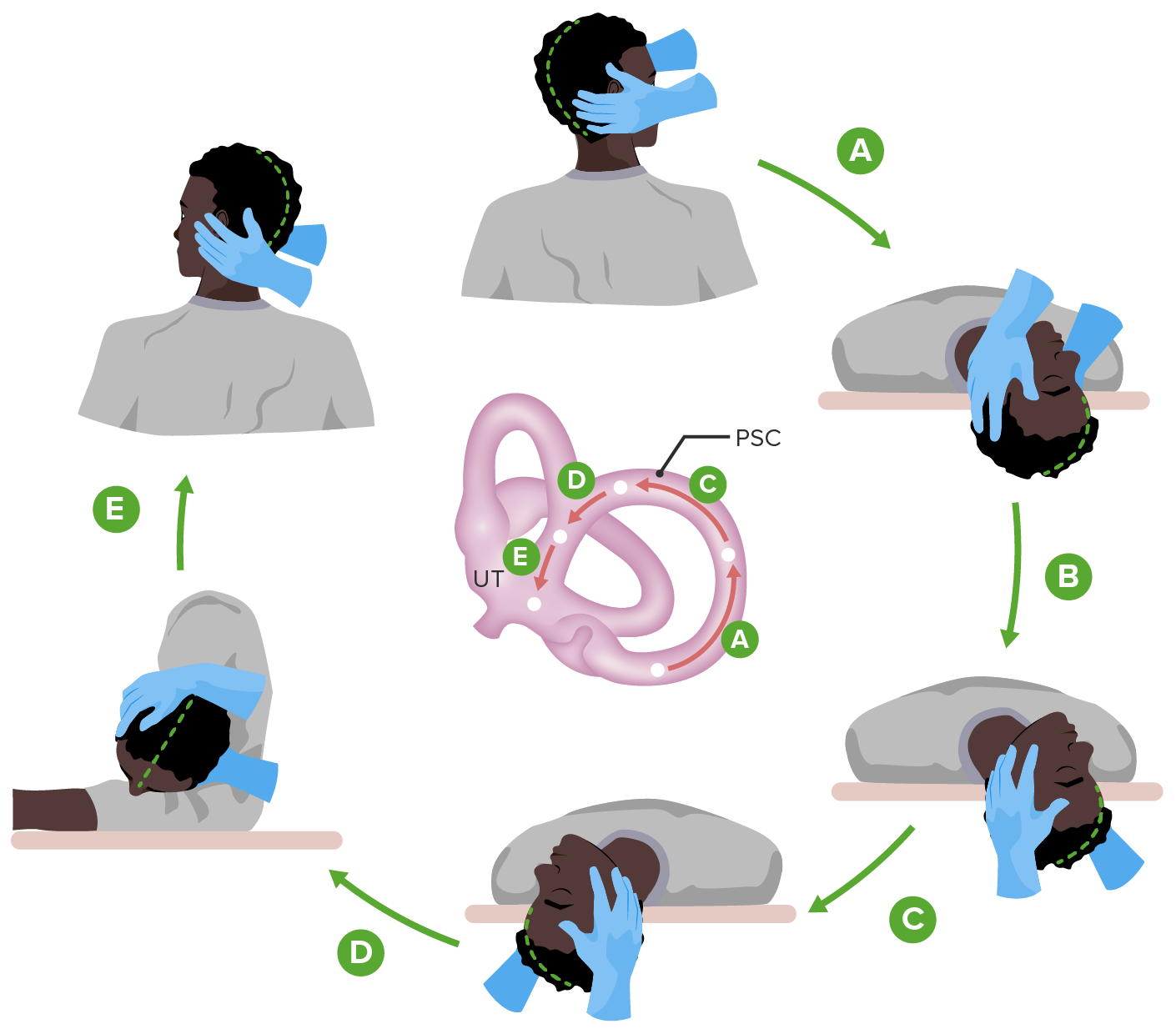
00:01 Let's talk more about our approach to vertigo. 00:04 Vertigo arises from a problem in the vestibular system. 00:07 And so we're going to start with understanding vestibular anatomy and use this to evaluate and ultimately to treat patients. 00:15 When we think about the vestibular system, it starts in the inner ear. 00:18 Information, sound waves, and airwaves come in through the external ear, are reverberated through the middle ear and received in the inner ear and the vestibular apparatus with the semicircular canals. 00:32 Those canals sense head movement, and are important for keeping our head, and eyes, and body all moving in the same direction. 00:40 From the inner ear and the vestibular apparatus, the vestibular nerve carries sensory afferents information about head movement to the brainstem. 00:49 And vestibular nerve function is critical for maintaining normal head and eye balance and preventing vertigo. 00:57 Those are the inputs to the system. 01:00 The system relays at the vestibular nuclei, which we'll talk about in the next slide. 01:04 And then there are three important outputs. 01:07 From the vestibular nuclei, information about head movement goes to the eyes in connecting to the ocular motor system, to the cerebellum to coordinate movement, and then down to the spine so that we can maintain good postural tone as our head is moving. 01:23 And problems with each one of those output circuits can contribute to vertigo or vestibular system pathology. 01:31 As we think a little bit more closely about that system, again, inputs arise from the labyrinth. 01:36 This is carried to the brainstem, through the vestibular nerve, to through cranial nerve eight, and the vestibular component of that vestibulocochlear nerve. 01:45 We see relays that go directly to the cerebellum. 01:48 And so the vestibular nerve communicates with the cerebellum through the flocculonodular lobe, and this is rapid communication to coordinate particularly head and eye movements. 01:58 But the dominant brainstem relay center is are the vestibular nuclei. 02:02 There are inferior and superior nuclei, a large relay center for all of this information. 02:09 The vestibular nuclei send information up through the medial longitudinal fasciculus and to coordinate with eye movements through cranial nerves three, four and six, so that when the head moves in one direction, the eyes move in the opposite and we can maintain fixation. 02:25 There's also descending outputs from the vestibular nuclei to the spinal cord to maintain postural tone as the head is moving both forward and backward, side to side and in a rotary fashion. 02:37 These descending outputs are primarily through the medial vestibulospinal track, and the lateral vestibulospinal tract. 02:44 Again, coordinating vestibular inputs with spinal outputs. 02:48 Problems anywhere along this circuitry can contribute to difficulty and patient symptoms that may present initially with vertigo. 03:00 But let's talk about how we evaluate patients if that's the underlying anatomy, and when that anatomy goes awry patients present with vertigo. 03:07 What do we do clinically, when we're seeing patients or evaluating vignettes to sort through the precise cause? The first is to understand the patient description. 03:16 We're looking for problems with vertigo with the vestibular system, not disequilibrium, or syncope presyncope. 03:23 Once we've honed in on a vestibular circuitry problem, our first step is to look at the time course. 03:30 What was the speed of onset of this condition? Was it acute like a stroke, subacute like many conditions are chronic, like an underlying degenerative or neoplastic problem. 03:40 And importantly, we want to look at the progression over time. 03:44 Some vestibular problems will present episodically as we saw in our case, others will progress, and some may be persistent. 03:52 And the evolution of the disease over time can be helpful for driving at the precise etiology, as we'll see. 03:58 The second feature of the history that we interrogate are any aggravating or alleviating factors. 04:04 And this is critical for evaluating patients with vertigo, where some causes of vertigo are positionally provoked, like BPPV and others are not.
About the Lecture
The lecture Review of the Vestibular System and Evaluation of Vertigo by Roy Strowd, MD is from the course Vertigo, Dizziness, and Disorders of Balance.
Included Quiz Questions
Which statement is the most accurate with respect to the vestibular system?
- The oculomotor system receives input from the vestibular system.
- Only a problem with the vestibular nuclei can cause vertigo.
- The inner ear, cochlea, and semicircular canals are not part of the vestibular system.
- The vestibular nerve carries efferent information from the brain.
- The vestibular system has a relay before its signals reach the flocculonodular lobe.
Which statement is the most accurate with respect to the vestibular system pathway?
- The medial and lateral vestibulospinal tracts help with postural control.
- Afferent signals go down the vestibulospinal tracts before they synapse in the vestibular nuclei.
- It supplies afferent information to cranial nerves III, IV, and VII.
- The flocculonodular lobe receives input from the vestibular nuclei.
Author of lecture Review of the Vestibular System and Evaluation of Vertigo

Roy Strowd, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
