Playlist
Show Playlist
Hide Playlist
Restrictive Cardiomyopathy

-
Slides Cardiomyopathy.pdf
-
Reference List Pathology.pdf
-
Download Lecture Overview
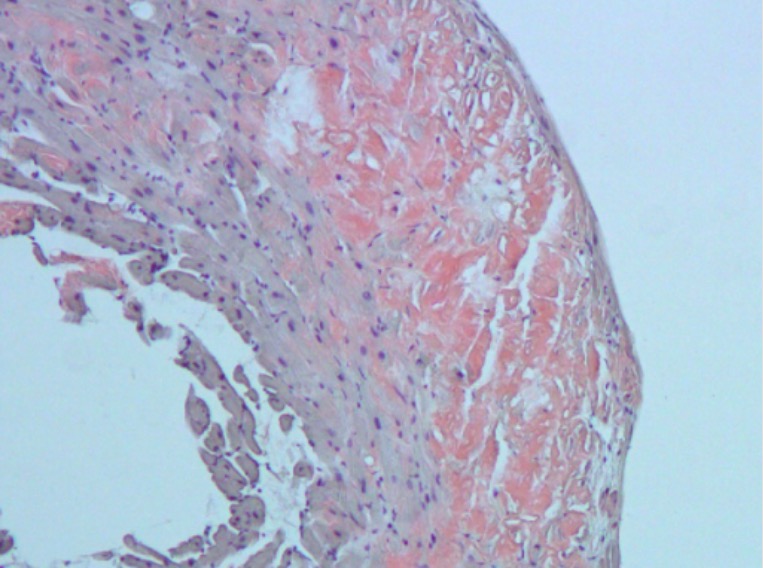
00:01 The final category of cardiomyopathy is restrictive cardiomyopathy. 00:05 Restrictive cardiomyopathies are fundamentally a diastolic dysfunction cardiomyopathy. 00:12 So in some respects, it share some of the features with hypertrophic cardiomyopathy. 00:16 Overall, it is the least common of all three types - dilated, hypertrophic and restrictive, about 5% overall, or less. 00:26 What's been indicated on the schematic is that the myocardium has been partially replaced with something else that isn't myocardium. 00:35 Fundamentally, this makes the wall less able to dilate and fill, it makes it stiffer. 00:42 As a result of that, we do not have normal filling of the left ventricle. 00:48 Sitting behind the left ventricle, his left atrium, it's trying to squeeze blood into that very stiff left ventricle and it's not being successful. 00:56 So you have a volume overload leading to dilation of the left atrium. 01:01 So in words, what I just said, you get stiffening of the ventricular wall, loss of myocardial flexibility, contractile force, due to infiltration by abnormal tissues. 01:13 This can also occur not only due to the infiltration with things like amyloid, but also due to scarring of the pericardium. 01:22 So that would be a constructive cardiomyopathy if we have fibrous connective tissue, completely surrounding the heart that will also keep the heart from being able to fill during diastole. 01:33 And we'll have a similar physiologic manifestation. 01:39 What are the causes? Like everything in medicine, idiopathic is always on your differential, meaning we don't know. 01:46 I suspect, as we get smarter and more clever and are able to do deep sequencing, we'll find more genetic basis for this. 01:55 There are various familiar forms of restrictive cardiomyopathy with known genetic mutations, we'll briefly touch on those. 02:04 But most commonly, as causes, restrictive cardiomyopathy are the deposition of other non-cardiac proteins. 02:14 Chief amongst these is amyloid. 02:16 We'll talk more about that. 02:17 But sarcoid can also be a cause of restricted cardiomyopathy. 02:21 If you've been paying attention, you're saying, 'Wait, you said sarcoid could be dilated cardiomyopathy? Yep, it can. 02:27 In some cases, because of the scarring and the deposition, you can also get a restrictive cardiomyopathy. 02:33 Hemochromatosis can also cause a restrictive cardiomyopathy. 02:38 Initially, it will prominently present as a dilated cardiomyopathy due to apoptosis due to iron overload, reactive oxygen species, et cetera. 02:47 But with time, you can get fibrosis so it can become a restrictive cardiomyopathy, And then Loeffler's endomyocarditis. 02:55 A rare but interesting form of restrictive cardiomyopathy due to thickening fibrosis of the endocardial layer. 03:05 In restricted cardiomyopathy, fundamentally, there's some increased extracellular material not otherwise specified in the myocardium. 03:13 Or you can have endocardial scarring, the lining of the ventricular walls become fibrotic. 03:21 That will also keep the wall from being able to fill during diastole. 03:26 You have decreased diastolic relaxation, and decreased ventricular filling, the consequences are due to a stiffened ventricular wall. 03:36 And upstream, we're going to get atrial dilation. 03:39 That poor atrium, left atrium is trying to squeeze blood into that stiff left ventricles like, can't get anywhere, so you get atrial dilation.. 03:48 With that happening, you can get systemic venous congestion. 03:53 Basically, the increased pressure and volume overload in the atrium reflects back through the lungs and into the systemic vasculature. 04:00 So you can see left heart failure, right heart failure, biventricular failure. 04:07 There's also diminished cardiac output. 04:09 Clearly, you're not filling the ventricles, so you're not getting the maximum amount of volume out so patients can also present with hypotension. 04:18 The configuration is different than what we saw in dilated or in hypertrophic cardiomyopathy. 04:23 This is not a floppy heart. 04:24 This is not a muscular heart. 04:26 This is kind of a normal-sized chamber, but the nature of what's in the walls makes it stiff. 04:34 The atria will dilate up, and that's an important component of a restrictive cardiomyopathy. 04:41 This is just showing you an example of restrictive cardiomyopathy due more to the endocardial fibrosis. 04:48 The wall may actually not have much in the way of extracellular material, but the endocardium being fibrosed limits the movement of that wall. 05:00 What are the signs and symptoms? Well, you can predict based on what you now know about the pathophysiology. 05:05 You have poor forward flow so patients are dizzy, lightheaded, they may have frank syncope. 05:10 They may have left heart failure, so they are dyspneic. 05:14 You can also, as part of that dyspnea and the pulmonary edema have rales. 05:19 You can also have diminished flow into the coronary artery, so you have angina and you can have arrhythmias. 05:26 So all the things again, kind of just because you have this doesn't necessarily mean that you have a restrictive cardiomyopathy. 05:33 Clearly it could be dilated cardiomyopathy, hypertrophic cardiomyopathy or some other cause. 05:40 But these are signs and symptoms associated with that. 05:43 And you may also see a systolic heart murmur. 05:47 So abnormal flow through the valve because of poor filling of the heart.
About the Lecture
The lecture Restrictive Cardiomyopathy by Richard Mitchell, MD, PhD is from the course Cardiomyopathy.
Included Quiz Questions
Restrictive cardiomyopathy is...
- ...ventricular wall stiffening that prevents the ventricle from stretching and filling with blood.
- ...ventricular wall thickening that prevents the ventricle from stretching and filling with blood.
- ...ventricular atrophy that prevents the ventricle from stretching and filling with blood.
- ...atrial wall stiffening that prevents the ventricle from stretching and filling with blood.
- ...atrial wall thickening that prevents the ventricle from stretching and filling with blood.
What pathophysiological change is seen with restrictive cardiomyopathy?
- Decreased diastolic relaxation
- Increased ventricular filling
- Decreased systolic contractility
- Decreased extracellular material in the myocardium
Author of lecture Restrictive Cardiomyopathy

Richard Mitchell, MD, PhD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
