Playlist
Show Playlist
Hide Playlist
Renal Patho-Embryology

-
Slides CongenitalRenalPathology.pdf
-
Reference List Pathology.pdf
-
Download Lecture Overview
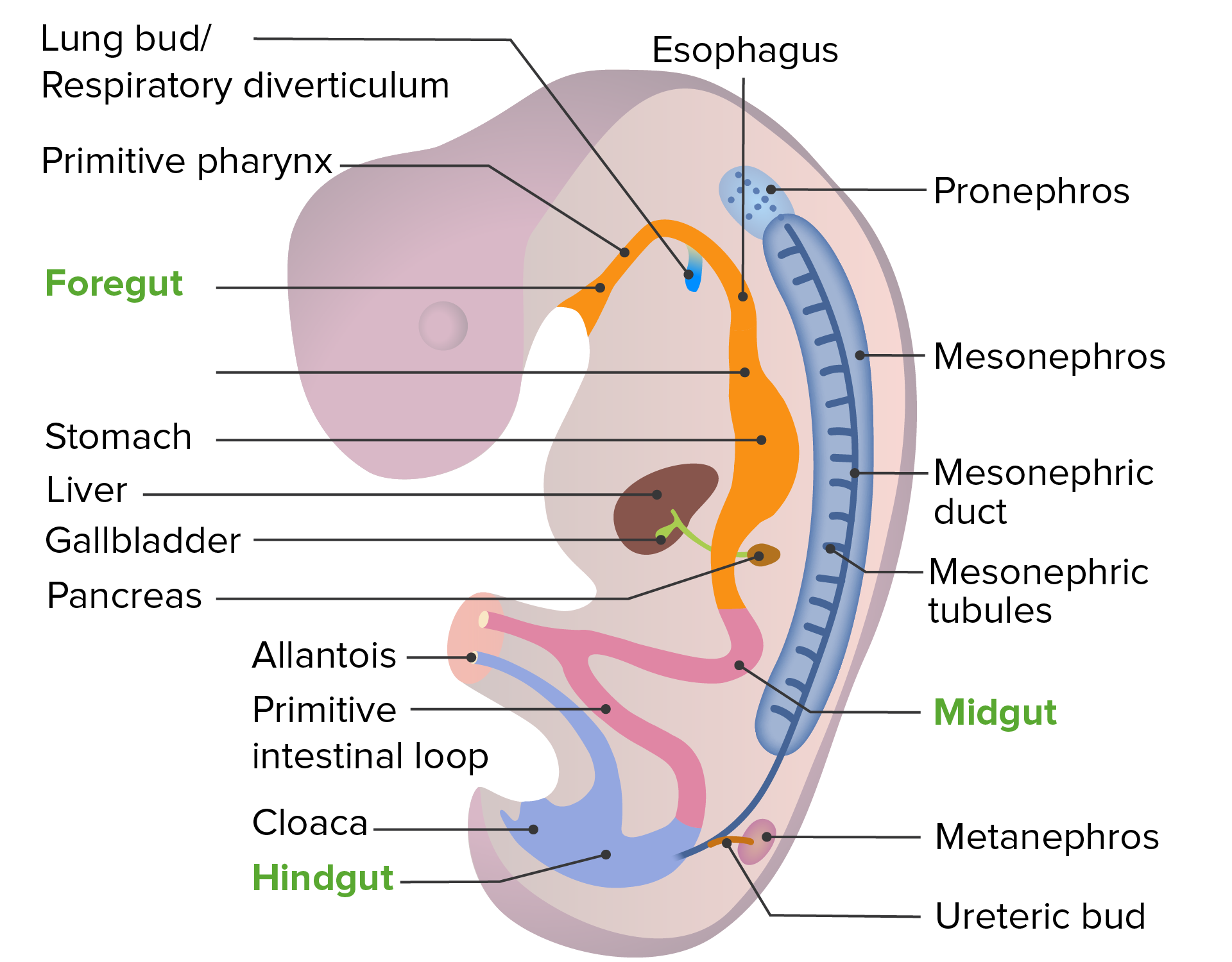
00:01 Let's take a look at congenital renopathology. 00:03 With embryology, there's certain components that we're going to derive so that we are able to give proper clinical relevance. 00:13 Now, from the top. Here we have an embryo and with this embryo, what exactly is going on? Well, what I'm trying to do here is make sure that you have a global picture as to where you can expect certain pathologies to appear and then when the time is right depending as to which organ system, we will dive into further detail if and when necessary. 00:37 But to begin with, number one, you see that? That is connecting to the outside world. 00:44 It's connecting the urinary bladder out into the umbilical cord. 00:50 Interesting. It's called allantois, and the remnant of it, urachus, if it was to remain. 00:58 At some point in time, if there is enough irritation taking place, there is a particular cancer that you can develop in the urinary bladder with the persistent urachus in which we then refer to as being, do you have any idea? It is not squamous cell cancer of your urinary bladder. 01:17 If it was smoking, you'll be transitional cell cancer of the urinary bladder because this is granular in nature, it would actually be adenocarcinoma of the urinary bladder. 01:27 Unbelievable, isn't it? You thought it was good enough just to know smoking and transitional cell cancer of the urinary bladder. 01:35 Not so much. 01:37 Maybe that in from microbiology that you wanna know about schistosomiasis and know that it's going to give rise to squamous cell cancer of the urinary bladder. 01:47 Well here, embryologically, a remnant of the urachus could result in pathologically, at some point in time, adenocarcinoma of the urinary bladder. Fascinating. 01:58 Abdominal wall, number two, and penis. We're thinking about the epispadias. 02:06 Stop there for one second. When we say epispadias, what does that refer to? That would be the top of the penis. What would you actually call that? The dorsum of the penis. 02:18 You want to use the same concept for the foot. When you dorsiflex, what is your foot doing? It's coming up like this, isn't it? Right? So, therefore, the dorsum of the penis, and if it was to be open, epispadias, then you're worried about a particular complication called urinary bladder exstrophy. E and E. 02:40 At some point, when we talk about hypospadias, a completely different discussion but that would be the ventral aspect of the penis. This is going to be dorsal. 02:51 I need you to know proper anatomical terminology. 02:55 Anus: imperforate. Meaning to say, if you have an imperforate anus, that could result in an interesting complications. 03:02 Now, the kidney. The kindey, there are a couple of things that I wish to point out to you: the metanephros that you're seeing here means that it is the permanent kidney. 03:12 T- metanephros, permanent kidney. 03:17 Whereas the mesonephros will be, well, we'll talk about this in the next bullet point here. 03:25 Then with the mesonephros, there would be more or less your interim. 03:29 But in the meantime though, the metanephros, permanently, and on the subsequent slide, I'll show you a picture of where the inferior poles of your kidney are then going to fuse together and it's actually more common than one would think. 03:43 Rendering the patient, susceptible with the kidney stones and the fact that it may get trapped underneath the inferior mesenteric artery. 03:51 Use the inferior pole as being the most common place of fusion as I show you along with the inferior mesenteric artery. 03:59 I and I, so that you have a point of reference. 04:03 Now, internal genitalia. Now, this is a wonderful discussion. 04:07 When the time is right, embryologically, of a condition called indigenous sensitivity syndrome, you might have known this being testicular feminization syndrome. 04:17 Androgen insensitivity syndrome is a much better clinical term and literally, the androgens are not able to properly work on the receptors. 04:27 Hence the name insensitivity. So what's happening? Well, if your antigen is not properly working on the receptor because that's the problem, then how in the world are you able to develop any of the proper male sexual structures? You cannot. This is the patient in which, well, phenotypically, he looks like a perfect phenotypic female and which upon pelvic examination, there is the vagina, but it ends up in a blind pouch because there isn't a uterus. 05:01 There are no ovaries and the gender sensitivity syndrome, what is your patient? Genotypically, a male. XY. Move on. Here we have abdominal wall. 05:12 What if you had an opening of the abdominal wall? Number 6, called omphalocele. 05:17 Urethra, hold on for one second, do not rush past this. 05:23 With urethra, embryologically or congenitally, say that you have a something called posterior urethral valves. 05:31 So think about where the urethra is. There's only one urethra. What do I mean? How many ureters do you have? Two ureters. Why am I bringing this up? Because say that you had posterior urethral valve issue in a young boy and what ends up happening? Urine is not moving forward. 05:52 If the urine isn't moving forward through the urethra, what will then happen? It'll back up. Back up into what? Urinary bladder. I want you to keep backing up into where? One or two ureters. Both bilateral urethral issues. 06:08 So, later on, when do male reproductive pathology and we further get into issues about -- have you've heard vesicoureteral reflux when the time is right and we'll talk about bilateral versus unilateral, urethral obstruction. 06:22 This is going to be a quite common young male with having bilateral-urethral issues. 06:29 Everything we just talked about here, one through seven, is going to be reviewed at some point in time. 06:36 But isn't it nice to have everything in one place where you can actually see as to how things are developing and giving it a clinical tag?
About the Lecture
The lecture Renal Patho-Embryology by Carlo Raj, MD is from the course Introduction to Renal Pathology.
Included Quiz Questions
Which of the following conditions results in vesicoureteral reflux in young boys?
- Posterior urethral valves
- Renal dysplasia
- Ureterocele
- Patent urachus
- Epispadias
Which of the following can lead to adenocarcinoma of the urinary bladder?
- Remnant of the urachus.
- Remnant of the anus.
- Remnant of the kidney.
- Remnant of the mesonephric duct.
- Remnant of the metanephric duct.
Which of the following terms is used to describe the opening of the penis on the dorsal side?
- Epispadias
- Urachus
- Posterior urethral valve
- Omphalocele
- Hypospadias
Author of lecture Renal Patho-Embryology

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
2 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Best lecture i have ever seen..concise with high yield topics.
Good very good,I like the lectures.Good very good,I like the lectures. Good very good,I like the lectures.
