Playlist
Show Playlist
Hide Playlist
Renal Losses: Metabolic Acidosis – Hypokalemia

-
Slides Potassium Disorders Hypo and Hyperkalemia.pdf
-
Reference List Nephrology.pdf
-
Download Lecture Overview
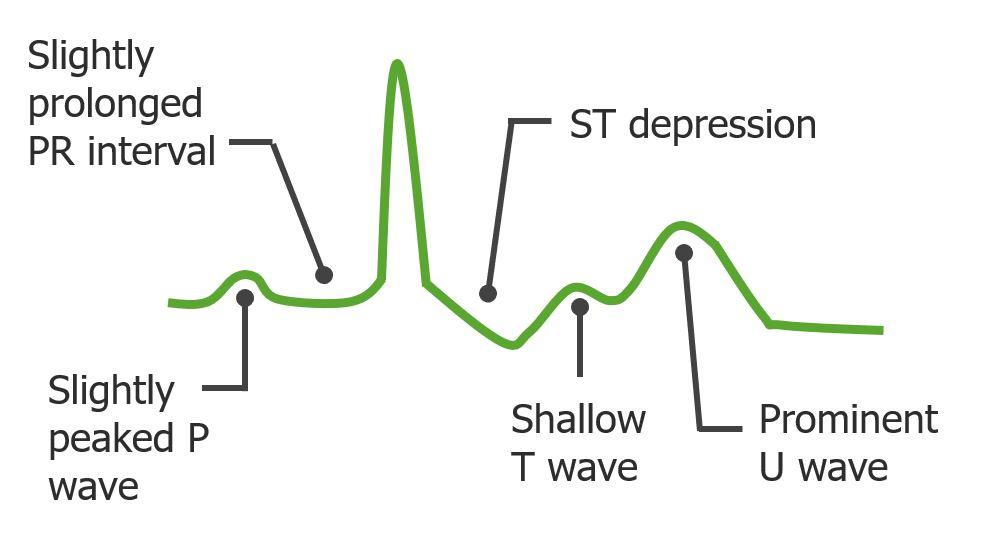
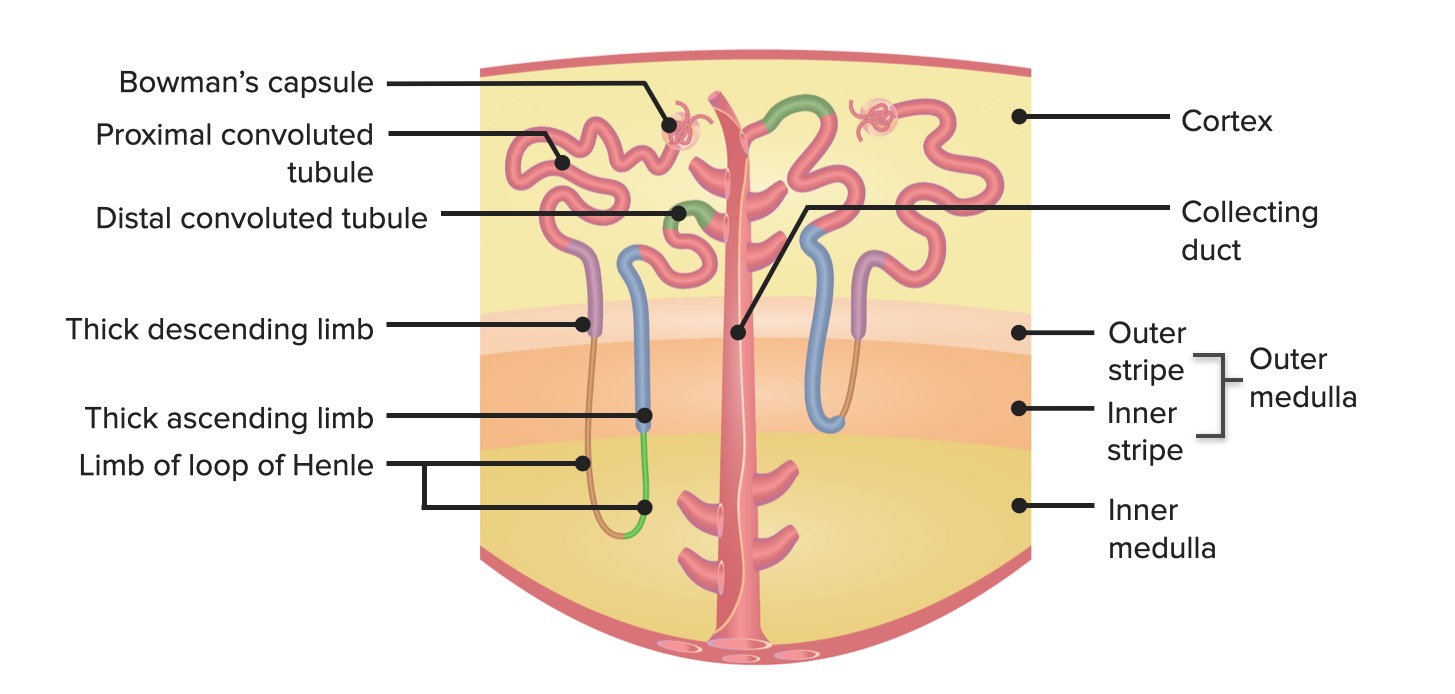
00:01 Now let's turn to hypokalemic disorders that present with a metabolic acidosis. 00:08 This includes things like renal tubular acidosis. 00:11 That is a hyperchloremic nonanion gap metabolic acidosis. 00:17 Now there's two main disorders that I want you to think about. 00:19 The first is a distal hypokalemic renal tubular acidosis or RTA. 00:24 That means it involves the alpha intercalated cell, which is at that collecting duct. 00:29 And it's then the distal portion of the Nephron. 00:32 You might also hear it referred to as a type 1 RTA. 00:36 And the problem here is really with impaired distal acidification. 00:41 So remember the alpha intercalated cell is being affected. 00:44 If that's the case then What that cell is supposed to do is it is the site of potassium reabsorption. 00:50 Remember there's a hydrogen ATPase at that apical region along with a hydrogen potassium ATPase. 00:57 And if I have mutations or if I have defects that affect either one of those I'm not going to be able to reabsorb potassium. 01:04 I also won't be able to distally acidify my urine which is why people end up with acid retention. 01:11 This can be due to things like familial disorders are autosomal disorders where you have mutations, either than in the hydrogen ATPase the hydrogen potassium ATPase or some of the basolateral transport proteins. 01:24 It can also be due to autoimmune diseases particularly Sjogren's disease. 01:29 Where you have problems with a hydrogen ATPase. 01:32 And then finally there are certain drugs like ifosfamide or others that can impact that hydrogen ATPase and that ability to reabsorb potassium. 01:41 And again, the mechanism here for hypokalemia is the fact that you are not able to reabsorb potassium at that alpha intercalated cell. 01:50 So the other RTA that I want you to think about is a proximal RTA or type 2 RTA. 01:57 So this is going to involve the proximal tubule and this involves a reduction in proximal tubular bicarbonate absorptive capacity. 02:06 So I want you to think about what happens normally. 02:10 The proximal tubule is the site of bicarbonate reclamation and we will filter and reabsorb all the bicarb in order to keep us in steady state. 02:18 That's typically a serum bicarbonate between 22 and 20 milliequivalents per liter. 02:22 When somebody has a proximal RTA it's either because the proximal tubular cells are damaged, they have a problem with carbonic anhydrase and when that happens they may only be able to absorb bicarb to the reabsorbed of threshold. 02:36 Maybe they'd get a serum bicarb between 14 and 16 Milli equivalents per liter. 02:41 Any bicarb that gets filtered beyond its threshold will not get reabsorbed and therefore will get filtered into the tubular fluid. 02:49 Now remember when you have bicarbonate wasting in the urine, then that is going to pair with sodium. 02:55 That sodium is going to be delivered distally to that principle cell and that is the mechanism of potassium e-flux. 03:03 So you're not always going to see hypokalemia in a proximal RTA. 03:07 You're only going to see it when that patient specifically has bicarbonate wasting. 03:13 Some of the causes of proximal RTA's or type 2 RTA's include familial causes. 03:17 So these are autosomal disorders. 03:20 We can also see this with multiple myeloma. 03:22 That's what I typically see in my adult population and this is because as people form these monoclonal immunoglobulin light chains, they get reabsorbed by the proximal tubule and if it's overly abundant it can damage those proximal tubular cells and they can end up with a proximal RTA we can also see this with certain drugs. 03:39 One of the big ones that again I see in my patient population is tenofovir which is one of our ART medications for HIV population. 03:48 Now the other category that I want you to think about that is associated with a metabolic acidosis and hypokalemia are non reabsorbable anions. 03:56 This includes toluene. 03:58 Toluene is found in paint thinner and it's actually used as a drug of abuse. 04:02 When people in just toluene it's metabolized so quickly to the form of hippurate that we actually won't see an anion gap acidosis even though it's an unmeasured anion. 04:13 It gets filtered by the kidney metabolized into hippurate. 04:16 And because hippurate is a non reabsorbable anion it is going to pair with sodium and when it does so then that is going to be delivered to our principal cell and favor potassium e-flux into that tubular fluid. 04:31 Diabetic ketoacidosis is also something that we have to think about in terms of having non reabsorbable anions. 04:36 Beta-hydroxybutyrate. 04:37 It's a non reabsorbable anion again, it's going to pair with sodium as it gets filtered into the urine that leads to an increase in distal sodium delivery and potassium e-flux into the tubular fluid.
About the Lecture
The lecture Renal Losses: Metabolic Acidosis – Hypokalemia by Amy Sussman, MD is from the course Potassium Disorders: Hypo- and Hyperkalemia.
Included Quiz Questions
Which of the following statements is true regarding distal renal tubular acidosis?
- It is associated with Sjogren syndrome.
- It leads to elevated serum chloride and potassium levels.
- It involves the principal cells of the collecting ducts.
- It is caused by defective bicarbonate absorption.
- It is caused by excessive hydrogen excretion.
Which of the following medications is associated with type 2 renal tubular acidosis?
- Acetazolamide
- Ifosfamide
- Thiazide
- Procainamide
- Spironolactone
Author of lecture Renal Losses: Metabolic Acidosis – Hypokalemia

Amy Sussman, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
