Playlist
Show Playlist
Hide Playlist
Rapid Squatting

-
Slides Heart Sounds Cardiovascular Pathology.pdf
-
Reference List Pathology.pdf
-
Download Lecture Overview
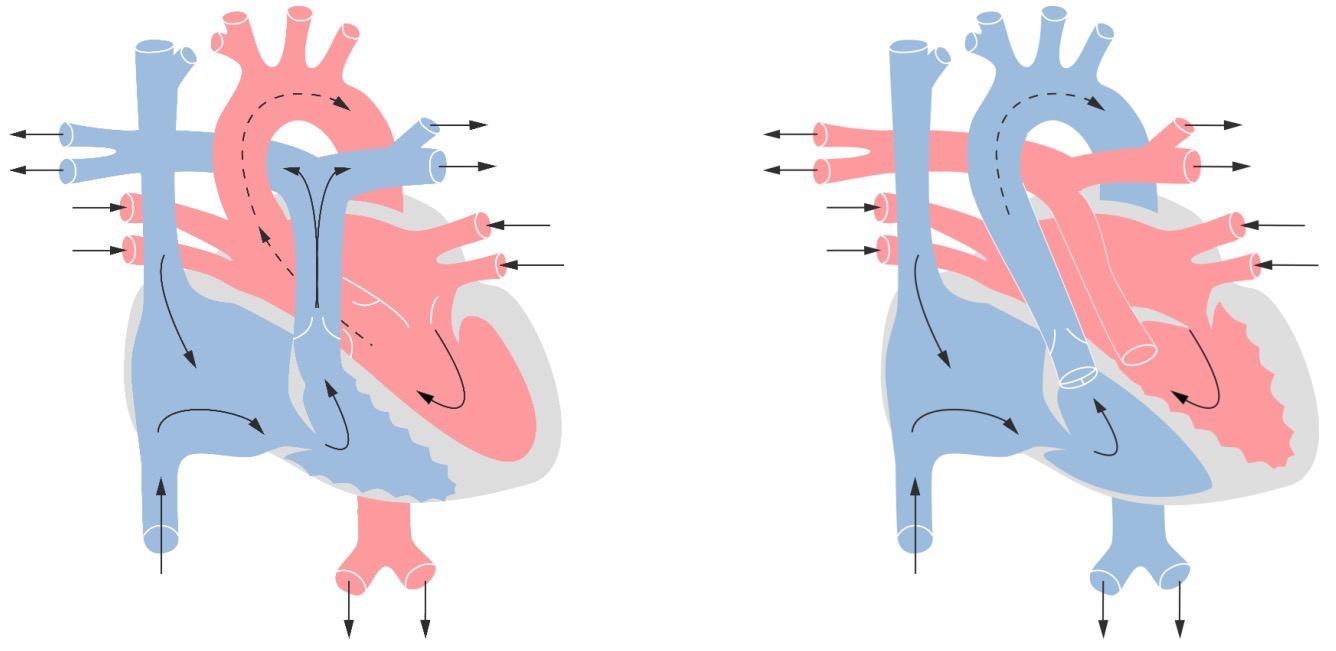
00:00 Last point here brings us to rapid squatting. 00:04 Couple of things that you want to keep in mind with rapid squatting. Well here is a maneuver that you as a clinician are perfoming or asking the patient to do to figure out as to what kind of murmur your patient might be suffering from. Or a maneuver that a child would be conducting to relieve a particular symptom that the patient might be feeling. 00:30 So what are we getting at here? With rapid squatting or squatting in general, what you want to do is you want to be able to delineate the two conditions in which squatting becomes beneficial for a clinician, in which you want to see us as to whether or not the intensity of the murmur is going to increase or decrease and you ask the patient to conduct rapid squatting, then blood will be returned to the heart in an increased fashion. Is that clear? Now what about this patient? Ready? It is a child, he'd love to play. "Mummy I want to go play." Play hide and seek and while at some point when the child is seeking that hiding place, the child gets tired and the child squats, but not to increase venous return. The child is instinctively squatting because the child feels tired. The child has hypoxemia. The child is experiencing cyanosis. The child might have pulmonic stenosis, right ventricular hypertrophy, ventricular septal defect. Those three will give you the clinical picture of your patient and what is that picture that I am referring to? Why those three? Pulmonic stenosis always begin there. Right ventricular hypertrophy and ventricular septal defect result in what kind of shunt in that case please? It is one of the most common congenital cyanotic heart disease and it is called tetralogy of Fallot. "But Dr. Raj you only gave me three, I thought tetra means four. Why being so foolish Dr. Raj?" Because I am giving you the three in which it gives you the clinical picture. What are those again? Number 1, pulmonic stenosis. Number 2, right ventricular hypertrophy. Number 3 was ventricular septal defect resulting in a right to left shunt, interesting. VSD in that case would be right to left because of the other predisposing issues. The fourth and final tetra would be the overriding aorta. Now why am I bringing this up? Because that squatting maneuver that the child was performing instinctively was then causing increased in TPR. Our discusison earlier with TPR was what? When you increase your TPR, what does it do to your afterload? Good. It increase afterload. If you increase that afterload, then what are you doing with the left ventricle? You're increasing the resistance to the left ventricle is facing. So now at this point, with that child feeling cyanotic, with the squatting maneuver is then going to reverse that right to left shunt to a left to right shunt. And by doing so, relieve some of the cyanosis. Is that clear? So we have squatting in two different conditions. What we have here is the fact that it increases venous return upon rapid squatting, so that will be to the right side of the heart through your veins. And then tetralogy of Fallot, that squatting would be conducted or performed to relieve the symptoms of your patient.
About the Lecture
The lecture Rapid Squatting by Carlo Raj, MD is from the course Heart Sounds.
Included Quiz Questions
Which of the following will cause a decrease in the venous return to the heart?
- Standing
- Deep inspiration
- Passive leg raise
- Supine position
- Sleeping
What occurs when a child squats during a "tet" spell?
- Reversal of the right-to-left shunt
- Reversal of the left-to-right shunt
- Decrease in the venous return to the heart
- Decrease in total peripheral resistance
- Decrease in afterload
Author of lecture Rapid Squatting

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Well, this a combined review of your heart sound & murmur series. I found them to be concise very high yield with a re-watchablity factor to it. very much appreciated your vigor enthusiasm gets me pumped. Some of the points you made were very complicated, i know you did your best if you could find mnemonics would be amazing and will push you forward. So far my favorite lecture here lol would definitely recommend your videos to friends. Thanks
