Playlist
Show Playlist
Hide Playlist
Posterior Urethral Valves (PUV) and Ureteropelvic Junction (UPJ) Obstruction


-
Slides VUR Pediatrics.pdf
-
Download Lecture Overview
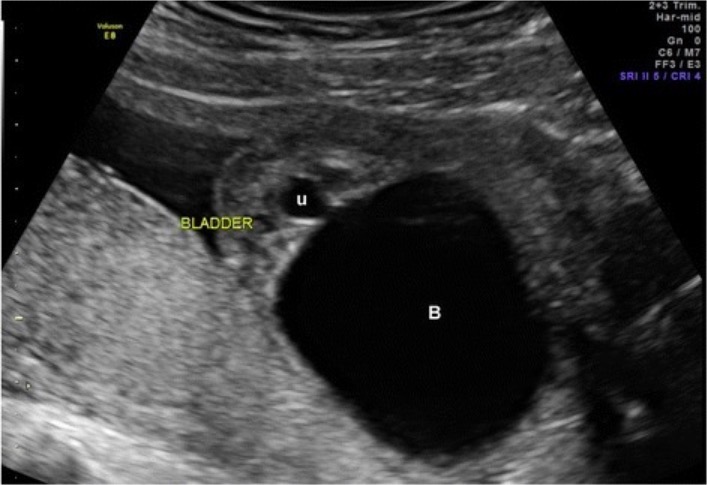
00:01 Here’s an example of posterior urethral valves. 00:04 This is a voiding cystourethrogram. 00:07 We have injected a dye into the bladder and now we’ve had the child pee while taking an x-ray. 00:14 Bear with me here because this might be a confusing picture for you. 00:18 This child has a mega ureter, a huge ureter as a result of longstanding vesicoureteral reflux. 00:25 You can see along the top that this huge ureter is going into what is really a distended bladder. 00:33 But the bladder needs to empty out in the body and it will go through the urethra. 00:37 If you notice at the outlet of this urethra, there is a little bit of a valve, but then there is this dilatation within the proximal urethra. 00:46 There are valves at the end of that. 00:49 This is not a true valve. 00:51 These are little flaps of tissue that are essentially acting like valves and preventing the urine from getting out of the bladder particularly well, so you see this distended bladder and vesicoureteral reflux. 01:04 This problem is more prevalent in infants who we call boys who dribble. 01:11 If you ask a parent who has had a baby boy, what’s it like when you see them pee? They’ll tell you, "He sprays all over the place." Most parents have been tagged with urine. 01:21 As they're changing the diaper, the baby pees that can go all over them. 01:25 This is a problem but in weird way it’s also consoling because you can be pretty confident that your baby boy does not have posterior urethral valves. 01:35 In babies with posterior urethral valves, they can’t generate that stream and the urine sort of dribbles out. 01:40 And parents usually have noticed this when you ask them. 01:43 These patients can have variable severity. 01:46 They may present in the perinatal period or shortly after birth with a total urinary obstruction. 01:53 Those kids can be very sick and they can develop peritonitis or even death if it’s not intervened with. 02:00 Or it can present much later on, say 5 years of age, with recurrent UTIs and you find that they had valves. 02:08 These patients generally will have abdominal distention. 02:13 Their bellies will bloat because of the giant bladder but perhaps also because of peritoneal involvement and they will tend to strain with urination. 02:25 So let’s look at how we would diagnose a posterior urethral valve if we suspected it. 02:31 Generally, we’ll start with an abdominal ultrasound. 02:34 Here’s an ultrasound we can see, and what you can see is this child has a very thickened bladder wall. 02:40 That’s a key finding in these patients. 02:43 Alternatively, we could get a voiding cystourethrogram like the one we showed previously that would show an outpouching and you would also see that thickened bladder wall. 02:52 The bladder wall is thickened because the child has been straining against that valve and it’s become a more muscular organ. 03:01 For posterior urethral valves, we’ll manage them by first correcting any electrolyte problems that maybe present and then we’ll generally just place a Foley catheter. 03:12 Sometimes getting that catheter through the first time can be problematic, may cause some blood and ironically, you could even fix the problem by ripping through those valves. 03:21 But we have to place this Foley because this child has to drain their urine. 03:26 Then later on or approximately, we’ll do a cystoscopic repair. 03:32 We’ll call our urology colleagues to come in and really fix the problem. 03:37 Afterwards, there’s a phenomenon called a post-obstructive diuresis. 03:41 Patients who’ve had an obstruction for a prolonged time maybe excessively diuretic afterwards so we have to take care of that. 03:50 These patients if they have renal damage may need dialysis or a transplant if there is substantial damage done. 03:59 Let’s switch gears to another secondary cause of vesicoureteral reflux. 04:04 This one is UPJ obstruction or ureteropelvic junction obstruction. 04:10 As that ureter is coursing in its retroperitoneal course just over the pelvic junction, it can kink. 04:18 This can cause a partial or total blockage of the urinary flow along that ureter and so the urine bounces back up into the kidney.
About the Lecture
The lecture Posterior Urethral Valves (PUV) and Ureteropelvic Junction (UPJ) Obstruction by Brian Alverson, MD is from the course Pediatric Nephrology and Urology. It contains the following chapters:
- Posterior Urethral Valves
- Ureteropelvic Junction (UPJ) Obstruction
Included Quiz Questions
Which of the following findings is most likely in an infant suspected of having posterior urethral valve?
- Weak urinary stream
- A hydrocele in the scrotum
- An indirect inguinal hernia
- Polycystic kidney disease
- A neurogenic bladder
A child with posterior urethral valve is least likely to present with which of the following?
- Persistent vomiting
- Urinary dribbling
- Straining with urination
- Abdominal distension
Which of the following is the most appropriate initial step in diagnosis when posterior urethral valve is suspected?
- Abdominal and pelvic ultrasound
- voiding cystourethrogram
- Abdominal CT scan
- Urine culture
- Renal MRI
A neonate is brought to the emergency department because he has not passed urine for 2 days. He is irritable. Vital signs are within normal range. Physical examination shows lower abdominal distention. You order serum electrolytes. Which of the following is the most appropriate next step in management?
- Placement of a foley catheter
- Sedation with diazepam
- Intravenous 0.9% saline
- Placement of a suprapubic urine catheter
- Hemodialysis
Author of lecture Posterior Urethral Valves (PUV) and Ureteropelvic Junction (UPJ) Obstruction

Brian Alverson, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Excellent lecture. This is a very important topic in pediatrics. Thank you!
