Playlist
Show Playlist
Hide Playlist
Pulmonary Embolism: Pathogenesis


-
Slides PulmonaryEmbolism RespiratoryPathology.pdf
-
Reference List Pathology.pdf
-
Download Lecture Overview
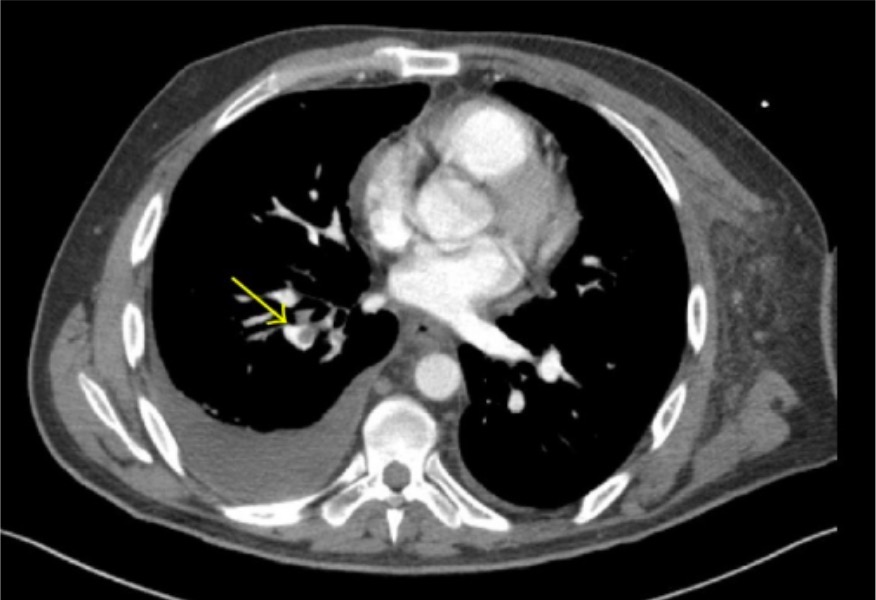
00:05 What is that? Rapid shallow breathing. 00:08 Welcome to pulmonary thrombi emboli. 00:10 So, with this, where does it begin? Disease process for the most part. 00:16 Well, if you're dealing with emboli, remember it's a moving thrombus, isn't it? Where do you think it's moving from and where did it originate from most likely? Well in our society, a venous thrombus, usually in the lower extremity and from henceforth, I'll abbreviate it as being LE or perhaps the pelvis. 00:35 But it begins as a DVT, a deep vein thrombosis. Then what happens? Oh my. 00:42 The thrombi starts breaking up a little bit, stop there for a second and you wanna start bringing your hemodynamics a little bit. 00:49 What do you mean? Well, how do you start breaking up a thrombi? The last time that you left your thrombus was fibrin, factor 13, and you have an insoluble clot. Isn't it? And so therefore, would you tell me as to which you require so that you can start breaking down this fibrin? Good. Plasmin. 01:09 So plasmin is a component that at some point, you have this thrombi sitting there in the deep, deep vein. 01:16 Risk factors will walk through and you start breaking down your fibrin. 01:20 Oh, what do you call that clinically? Oh my goodness. There's D-Dimer. Huh? There's your D-Dimer. 01:29 So, what it is, is basically your thrombin that's breaking up, in all means. 01:34 Okay. Is that something that you expect to find with the pulmonary embolus? Yeah, it is. Fantastic. 01:39 So you just knocked out two birds with one stone, most likely originating from your deep vein, down maybe perhaps in your deep vein in your leg, but also a deep vein in your thigh or sometimes your femoral vein. 01:53 And keep that in mind, it doesn't always have to be down in the leg and you don't necessarily have that - have to have that pain upon dorsiflexion. 02:01 Homans' sign that you all are quite familiar with if that gives it - if the boards or if the question gives that to you, fantastic. 02:09 I mean you know right off the bat that the patient needs to be put on a blood thinner. 02:13 We'll talk more about management later on. 02:16 So, just with that first statement there or first paragraph, you understand as to what's going on with your PE or pulmonary thromboemboli. 02:23 Pulmonary embolus also increase the vascular resistance as you can imagine and so therefore, who's gonna suffer this type of resistance? Good. The right ventricle. 02:34 Let's continue. Now, sufficient large PEs can lead to circulatory collapse. 02:38 Uh-oh. Right ventricle dies as do you, you don't want this. 02:44 This embolus is known as a saddle embolus, it's huge, it's - did you have a sausage this morning by chance? If you did, imagine that sausage being in your pulmonary vasculature. 02:54 Could you imagine that being there? It just traveled up - no obviously, I'm exaggerating. 03:00 But these are huge saddle emboli and those are the ones that you wanna pay attention to in terms of your clinical vignettes and questions because this is then associated with increased morbidity, mortality. 03:14 It's a life threatening emergency. Are we clear? On the CT here, we're seeing a pulmonary embolus that's massive, it's large. 03:25 It’s called a saddle embolus and has the circulatory consequence of hypotension and the respiratory consequence of hypoxia. 03:33 When more peripheral pulmonary arteries are involved (as shown in the schematic here where the left lower lobar artery is involved by an embolus), the area of subtended lung may be infarcted, which appears as a wedge-shaped density on chest X-ray. 03:51 However, infarction is not common in pulmonary embolism because of 3 non-redundant pulmonary oxygenation sources: The pulmonary arterial circulation (venous blood), The bronchial circulation (arterial blood), and direct alveolar ventilation via alveolar pores and/or airway anastomoses
About the Lecture
The lecture Pulmonary Embolism: Pathogenesis by Carlo Raj, MD is from the course Disorders of the Pulmonary Circulation and the Respiratory Regulation: Basic Principles with Carlo Raj.
Included Quiz Questions
Which factor is required in order to break down an insoluble clot?
- Plasmin
- Fibrin
- Von Willebrand factor
- D-dimer
- Vitamin K
Which of the following signs would increase the suspicion for deep vein thrombosis?
- Pain on dorsiflexion of the lower extremity
- Bronchial breath sounds
- Bilateral pitting edema of the lower extremities
- Throbbing of the femoral artery on palpation
- Pain on inspiration with palpation
Author of lecture Pulmonary Embolism: Pathogenesis

Carlo Raj, MD
Customer reviews
1,0 of 5 stars
| 5 Stars |
|
0 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
12 |
12 customer reviews without text
12 user review without text
