Playlist
Show Playlist
Hide Playlist
Pulmonary Embolism: Diagnosis



-
Slides PulmonaryEmbolism RespiratoryPathology.pdf
-
Reference List Pathology.pdf
-
Download Lecture Overview
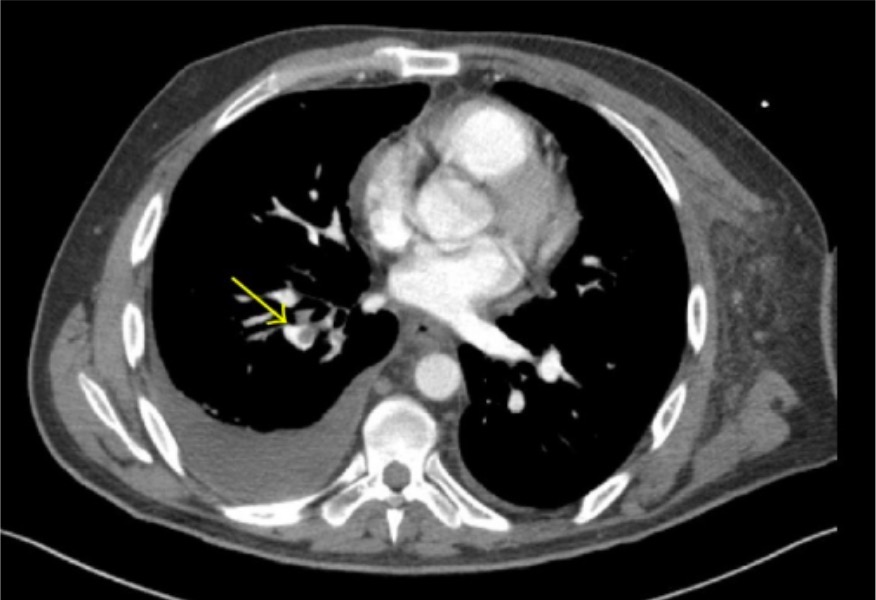
00:00 This lecture is about making the diagnosis of Pulmonary Embolism or PE. 00:06 This condition can be life-threatening, and early and accurate diagnosis is crucial. 00:11 We will explore the methods and tools at our disposal to diagnose PE effectively. 00:16 Diagnosis of PE involves a comprehensive approach, which includes clinical assessment, laboratory testing, and imaging studies. In this lecture, we'll primarily focus on the clinical assessment aspect of PE diagnosis. 00:31 One of the first steps in diagnosing PE is to assess the patient clinically. 00:36 To aid in this assessment, we can utilize a validated pre-test probability (PTP) score. 00:41 The Wells score is a commonly used tool in this context. 00:45 It helps us gauge the likelihood of a patient having a PE based on various clinical factors. 00:51 It is not necessary to memorize the criteria for board examinations, but you should be aware of how the score is used. 00:58 For those who want to memorize them, one mnemonic is "TINT HIP." Here are the components of the Wells score: Tachycardia a pulse over 100 assigns 1.5 points. An elevated heart rate can be indicative of PE. 01:14 Immobilization or surgery 3 or more days also assigns 1.5 points. Immobilization or recent surgery can increase the risk of PE. 01:24 No alternative diagnosis assigns 3 points. This is crucial; if there is no other plausible explanation for the patient's symptoms, it raises suspicion for PE. 01:34 Tenderness (calf or thigh) - Assigns 3 points. Tenderness in the calf or thigh can suggest deep vein thrombosis (DVT), a common precursor to PE. 01:46 History of DVT or PE. This assigns 1.5 points. A previous history of DVT or PE increases the likelihood of recurrence. 01:55 Hemoptysis assigns 1 point. Hemoptysis, or coughing up blood, can be a symptom of PE. The presence of malignancy assigns 1 point. Malignancies can increase the risk of developing blood clots. 02:09 Now that we have discussed the Wells score and its components, let's move on to how we utilize this information to guide our diagnostic process. The simplified two-tiered clinical probability score is a practical tool for decision-making in suspected PE cases. 02:25 If the total Wells score is low (less than or equal to 4.0), PE is considered unlikely. 02:32 However, we take an additional step by performing a D-dimer test. It’s essential to note that D-dimer levels can be elevated for various reasons. 02:41 If the D-dimer result is low (less than 500 nanograms/mL), no further testing for PE is required, and we can rule it out. 02:49 If the D-dimer result is high (greater than 500 nanograms/mL), the next step is to proceed with a CT pulmonary angiogram (CTPA), unless this imaging modality is unavailable, in which case a V/Q scan can be considered. 03:06 Conversely, if the total Wells score is high (more than 4.0), PE is considered likely. 03:12 In such cases, we proceed directly with a CT pulmonary angiogram (CTPA), unless a V/Q scan is the only available option. 03:19 This is one approach to diagnosing PE, but in the medical field, it's important to acknowledge that there can be variations in the decision-making process, and clinical judgment remains paramount. 03:32 These scoring and decision criteria provide us with a systematic approach to evaluate the likelihood of PE, enabling us to make informed decisions and promptly initiate appropriate interventions. 03:47 Here is a CTPA, demonstrating a large saddle embolus, it’s extending into the right and left pulmonary arteries. 03:54 Note that the Pulmonary artery is filled with contrast dye which appears white. 04:00 The saddle embolus appears gray and is called a filling defect because it blocks the filling of that part of the artery. 04:08 In summary, the combination of clinical assessment, pre-test probability score, and the D-dimer helps determine the likelihood of PE. 04:17 Then appropriate imaging studies are conducted based on the pre-test probability and D-dimer results. 04:24 Besides diagnosis, it is important to be aware of additional Clinical factors: In addition to the scoring system, we must consider the clinical symptoms and signs that may accompany PE. 04:36 These can vary widely among patients, and it's crucial to maintain a high index of suspicion. 04:43 Here are some key signs and symptoms, and the percentage of time they are present: The symptoms may also present asymptomatically Dyspnea at rest or with exertion (73%), Pleuritic pain (66%), Cough (37%), Orthopnea (28%), Calf or thigh pain and/or swelling (44%) Signs: Calf or thigh swelling, erythema, edema, tenderness, palpable cords (47%) Tachycardia (24%), Rales (18%), Decreased breath sounds (17%) ECG abnormalities are common but nonspecific in PE cases. They may include: Tachycardia Nonspecific ST-segment and T-wave changes in approximately 70% of cases "Classic" abnormalities, such as the S1Q3T3 pattern (i.e., S wave in lead 1, Q wave in lead 3, and inverted T wave in lead 3), right ventricular strain, and incomplete right bundle branch block, are less common but associated with a poorer prognosis. 05:56 Chest X-rays can reveal abnormalities such as atelectasis or effusion, but these findings are also nonspecific. 06:05 Approximately 20% of patients with PE may have normal chest X-rays. 06:11 However, a chest X-ray can be valuable in identifying alternative causes of a patient's symptoms. 06:18 In cases where the patient is hemodynamically unstable, performing a CTPA is not advisable due to the patient's compromised condition. 06:27 Instead, our focus shifts to bedside lower extremity ultrasonography (to look for deep vein thrombosis) and transthoracic echocardiography (to look for new right ventricular strain or direct visualization of thrombus within the heart), which can provide a presumptive diagnosis of PE, even if these tests are not definitive proof. 06:52 For such patients, immediate thrombolysis may be justified to address the life-threatening nature of the condition. 07:00 In summary, the diagnosis of PE involves a multidimensional approach that integrates clinical assessment, scoring systems like the Wells score, and further diagnostic steps based on pre-test probability and D-dimer results. 07:15 Clinical symptoms and signs, along with ECG and chest X-ray findings, provide additional insights. 07:23 In critically ill patients, a different approach may be necessary to ensure timely intervention.
About the Lecture
The lecture Pulmonary Embolism: Diagnosis by Carlo Raj, MD is from the course Disorders of the Pulmonary Circulation and the Respiratory Regulation.
Included Quiz Questions
What is the classic ECG pattern associated with pulmonary embolism?
- S1Q3T3
- S3Q1T1
- Widened QRS
- New onset delta wave
- Polymorphic p waves
Which of the following statements regarding CT pulmonary angiography versus conventional catheter-based pulmonary angiography is CORRECT?
- CT pulmonary angiography allows for the identification of other lung pathologies.
- CT pulmonary angiography is more time-intensive
- Conventional catheter-based pulmonary angiography is less invasive.
- Conventional catheter-based pulmonary angiography is more cost-effective
What is the best first imaging test for suspected pulmonary embolism?
- CT pulmonary angiography
- CXR
- V/Q Scan
- CT chest without contrast
Author of lecture Pulmonary Embolism: Diagnosis

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
