Playlist
Show Playlist
Hide Playlist
Pseudogout (CPPD)


-
Slides Gout.pdf
-
Reference List Rheumatology.pdf
-
Download Lecture Overview
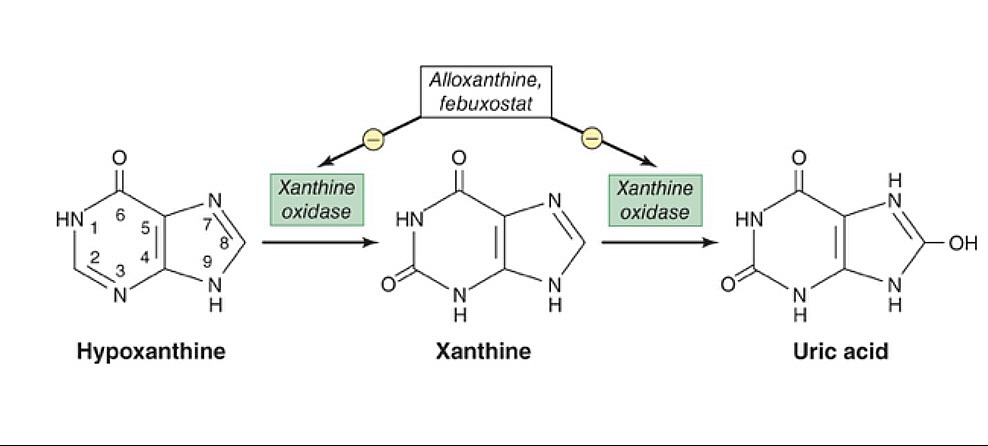
00:00 We should touch base just a little bit about Pseudogout since we've made mention of it and it is a crystalline arthropathy. 00:07 It has a lot of similar features to gout and we'll go through them very quickly. 00:10 So CPPD stands for calcium pyrophosphate crystal deposition. 00:16 It's called 'pseudogout' because it looks a lot like gout but it is a different disease process. 00:21 Risk factors are similar. 00:23 It's gonna be in elderly patients. 00:25 The differences are that these are folks who have hyperparathyroidism oftentimes or perhaps excess iron like hemochromatosis or too little phosphate or magnesium. 00:36 They're just different in some of the risk factors that we saw for gout Unlike gout which can most commonly cause podagra, again of the first MTP, pseudogout has a predilection for larger joints like the knees and perhaps the wrists. 00:51 The joint fluid, rather than finding those negatively birefringent needle-shaped crystals, for pseudogout, you're gonna see weakly positive birefringent rhomboid-shaped crystals that we'll take a look at on the next slide. 01:05 Sometimes, you may perform x-ray of particular joints that are involved then you might see some chondrocalcinosis which simply means calcific deposits in the cartiage. 01:14 The treatment of acute pseudogout by the way, is pretty similar to the treatment of gout acutely. 01:19 You're trying to decrease the inflammatory process. 01:22 NSAIDS, Colchicine, potentially intraarticular or systemic steroids. 01:27 The trouble with pseudogout is that for a long term management, you don't have things like allopurinol or uricosuric agents. 01:35 So you have fewer options to treat the pseudogout. 01:38 Though sometimes, people do use low dose Colchicine to reduce flares in the future Here's a picture of those crystals that we talked about. 01:46 You can see that they are more rhomboid in shape but they are also birefringent on polarized light. 01:53 With that, let's just highlight a few of our keypoints from gout again. 01:58 Again, it's caused by deposition of proinflammatory crystals in the synovial tissues. 02:04 There's an abrupt onset especially for early onset cases. 02:09 It's an abrupt case of monoarticular inflammation with pain, swelling, fluid in the joint. 02:17 The diagnosis will require synovial fluid analysis both to confirm the diagnosis and also to exclude other pathology like septic joint. 02:25 And the treatment acutely is gonna be Colchicine, NSAIDS, potentially intraarticular steroids and then we're gonna focus on prevention after that initial flare. 02:34 Risk factor modification: cut out all of that seafood, meat, alcohol, etcetera. 02:39 try and use some uric acid lowering medications like Probenecid or Allopurinol and those are basically the strategies that we'll use to decrease future episodes of gout.
About the Lecture
The lecture Pseudogout (CPPD) by Stephen Holt, MD, MS is from the course Non-Autoimmune Arthritis.
Included Quiz Questions
Which of the following conditions is commonly associated with pseudogout?
- Hemochromatosis
- Lesch-Nyhan syndrome
- Tumor lysis syndrome
- von Gierke disease
- Glucose-6-phosphatase deficiency
Author of lecture Pseudogout (CPPD)

Stephen Holt, MD, MS
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
1 customer review without text
1 user review without text
