Playlist
Show Playlist
Hide Playlist
Posterior Compartment of Leg

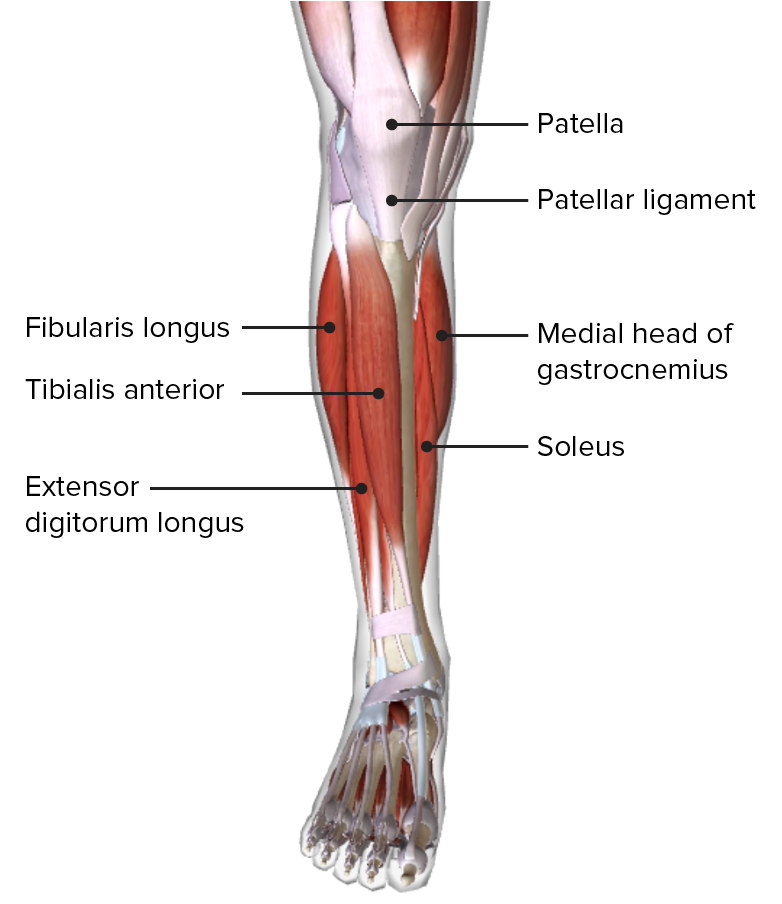
00:00 What about the posterior compartment of the leg? Yeah, so you have superficial and deep. 00:07 What is in the superficial part? Gastrocnemius. 00:10 Soleus, gastrocnemius, soleus. 00:12 Plantaris. 00:13 Plantaris, so these are the three superficial ones. 00:15 And deep ones? Tibialis posterior. 00:24 Flexor digitorum longus, flexor halluces longus and popliteus. 00:32 So seven muscles, three are superficial and four are deep. 00:36 Gastrocnemius, soleus, and plantaris are all superficial. 00:40 Tibialis posterior, flexor hallucis longus, flexor digitorum longus and popliteus are deep. 00:46 They're all supplied by the tibial nerve. 00:49 So if the tibial nerve is injured, then the patient is unable to plantar flex the foot, quite an important action. 00:57 The four muscles were flexor digitorum longus, flexor hallucis longus tibialis posterior and popliteus. 01:08 If the sciatic nerve is injured, then clearly, patient is unable to flex the knee and the entire angle is gone, no flexion, no dorsiflexion, no plantar flexion, no inversion, eversion. 01:24 That's the level of nerve injury. 01:25 Now, I mentioned about the popliteal artery. 01:29 Remember, I told you it comes off there from the Hunter's canal, it comes to the posterior compartment. 01:36 That's the popliteal artery. 01:38 Then classically, it trifurcates, or it can bifurcate. 01:43 When I say trifurcation, it divides into anterior tibial, posterior tibial, and peroneal. 01:52 Posterior tibial, as the name says, posterior to the tibia and accompanies the tibial nerve. 02:01 Anterior tibial accompanies the deep peroneal nerve. 02:08 It comes all the way up to the dorsum, to the anterior aspect of the angle joint and continues as the dorsalis pedis. 02:17 Posterior tibial runs in the posterior surface, turn around that way for a minute, and runs behind the medial malleolus. 02:26 I’m sure you know where the posterior tibial is. 02:29 So those are your artery, nerve, and vessel. 02:32 You can sit down now. 02:34 In summary, you can sit, thank you. You can sit down now. 02:34 In summary, you can sit, thank you. 02:37 In summary about the lower limb, four compartments. 02:40 You need to know what is in each compartment, what nerve, what artery, and what muscles. 02:47 Do you want to just take about 20 seconds to think about the muscles in each compartment, and the nerve, and the artery? In the ankle, the other thing we need to remember is you have the tibia and the fibula. 03:39 What's a bone on that? Talus and the calcaneus. 03:44 One of the questions they ask is where do you have dorsiflexion of the foot? Do you have in the ankle joint or the subtalar joint? Tibiotalar joint, that's where you get the dorsiflexion and plantar flexion. 04:00 So in the subtalar joint, you get inversion and eversion. 04:06 Weber’s fracture, you may be asked. Yes, Weber’s fracture can be asked. 04:13 Weber’s fracture is quite easy to remember. 04:24 So that's the tibia, fibula. Weber 1 is below the syndesmosis, Weber 2 is at the level, and Weber 3 is above. That’s all, 1, 2, and 3. 04:43 Do you want to think of anything else? We have covered everything we have to do on that. 04:56 Do you want to look at any question, anything you want to or you're unsure of? Origin and insertion of lower leg, you’re right. 05:14 Which one? All of them. 05:16 No, there are few things. You probably need to remember a little bit. 05:22 One is on the middle side of the foot here, middle side of the tibia, you have something called the pes anserinus. 05:31 What are they? Semitendinosus, semitendinosus, gracilis, and sartorius. 05:37 So say grace before tea. 05:38 So first is sartorius, gracilis, semitendinosus. So these are the three here. 05:44 On the lateral side, you have the biceps femoris attaching to the head of the fibula. 05:49 On the medial side, you have the semimembranosus, semitendinosus. 05:52 Those are the things. 05:54 Tibialis anterior and posterior, where do they attach? It's attached to the medial cuneiform, here on the middle side. 06:04 You don't really have to, I don’t, I haven't really seen that much sporadic about origin and insertion. 06:10 Nerve supply - probably they’ll give you a bone or give you the articulated foot. 06:20 Hello Johnny, thank you very much for your time. 06:22 Hope you enjoyed it. 06:22 Give him a warm applause, guys.
About the Lecture
The lecture Posterior Compartment of Leg by Stuart Enoch, PhD is from the course Upper Part of the Body Anatomy.
Included Quiz Questions
Which of the following structures passes through the diaphragmatic hiatus at T10?
- Esophagus and anterior and left vagus nerve
- Trachea and vagus nerve
- Esophagus and left phrenic nerve
- Right vagus
Which spinal level corresponds to the transpyloric plane?
- Lower border of L1 vertebra
- Upper border of L1 vertebra
- Lower border of T10
- Upper border of L3
The splenic plane can be found in which of the following areas?
- Transpyloric flexure
- Transesophogeal flexure
- Anterior mediastinum
- Left lower quadrant
A 16-year-old presents after being hit by a bat at spinal levels T10-T12. He complains of pain, bruising and difficulty performing daily functional activities. Which of the following organs is most likely injured?
- Kidneys
- Heart
- Gallbladder
- Lungs
Which of the following conditions is the most common cause of secondary hypertension?
- Renal artery stenosis
- Renal vein stenosis
- Diabetes
- Alcohol abuse
A surgeon makes a vertical incision for abdominal surgery. First, cutting into the rectus sheath at the inferior border posteriorly. What is the name of this incision point?
- Arcuate line
- Inguinal ligament
- Linea alba
- Falx ligament
A patient undergoes surgery in which palpation and incision of a deep fibrous fatty layer is performed. Which of the following structures was most likely incised?
- Scarpa’s fascia
- Camper’s fascia
- Subcutaneous tissue
- Peritoneum
Which of the following layers is deep to the internal oblique muscle, aids in the compression of the ribs and viscera and is the most engaged in strengthening exercises?
- Transverse abdominal muscle
- Pyramidalis muscle
- Peritoneum
- Fascia
Which of the following areas would not be crossed by incisions made below the arcuate line?
- The posterior rectus sheath
- Anterior rectus sheath
- Inferior rectus sheath
- Fascia
A patient comes in for inguinal hernia repair. The surgeon must palpate the area of the ligament before incision. The ligament can best be palpated from which of the following areas?
- The pubic tubercle to the anterior superior illac spine.
- The pubic tubercle to the inferior illiac spine.
- T10 to the anterior inferior illiac spine.
- The PSIS to the anterior superior illiac spine.
A patient was shot in the abdomen resulting in profuse bleeding from the structure which supplies most of the blood to the gut. The surgeon has to do an immediate operation and must identify the damaged artery. At which of the following spinal levels can this structure can be found?
- Lower border of T12
- Upper border of T10
- Lower border of L1
- Upper border of T12
Which of the following structures is not a branch of the celiac trunk?
- Right gastric artery
- Common hepatic artery
- Splenic artery
- Left gastric artery
A patient presents with a complaint of severe abdominal pain. On physical exam, the abdomen is tender to touch, with pain out of proportion. Imaging shows injury to the small intestines. Which of the following could be responsible for the above condition?
- Thrombosis of the superior mesenteric vein.
- Thrombosis of the inferior mesenteric artery.
- Thrombosis of the superior mesenteric nerve.
- Thrombosis of the inferior mesenteric nerve.
A patient comes in with severe portal hypertension and complains of lower abdominal pain. Which structure is most likely to be affected due to the patient’s condition?
- Superior rectal vein
- Inferior rectal vein
- Middle rectal vein
- Posterior rectal vein
A 46-year-old male with a known history of alcoholism develops severe cirrhosis leading to the appearance of bruises on his stomach in a striped pattern, esophageal varices and hypertension. The doctor discovers congestion within an anastomosis. Which of the following structures is most likely affected by portal hypertension leading to these signs?
- Left gastric vein and azygos vein
- Right gastric vein and colic vein
- Azygos vein and superior rectal vein
- Paraumbilical veins
A 72-year-old male patient is diagnosed with adenoma of the colon. He undergoes a procedure to remove right sided polyps near his cecum. The surgeon performs a right hemicolectomy. Where would the incision points most likely be made?
- Cecum to ⅓ of the transverse colon
- Rectum to ⅓ of the ascending colon
- Cecum to ⅔ of the transverse colon
- Rectume to ⅓ of the transverse colon
A small adenoma was found in the transverse aspect of the colon. The patient decides to undergo resection to prevent further spread. Which of the following is the best procedure to perform?
- Extended left hemicolectomy
- Right hemicolectomy
- Transverse colectomy
- Sigmoidectomy
Reanastomasis of an 85-year-old female after a right hemicolectomy, can be achieved the least invasively by which of the following procedures?
- Loop colostomy
- Total colonectomy
- Sigmoid colostomy
- Cecum colostomy
A 56-year-old female complains of constant lower abdominal and pelvic pain after an injury. She states a history of having a weakened structure in her injured inguinal canal. Which structure is the most likely cause of her discomfort?
- Round ligament
- Spermatic cord
- Femoral vein
- Femoral artery
The Inguinal canal is bordered by all of the following structures except?
- Rectus Abdominis
- external oblique
- inguinal ligament
- transversalis fascia
A 50-year-old man undergoes an abdominal hernia repair. The hernia is easily reducible and the contents could be pushed back through the external ring. The hernia falls superior to the inguinal ligament and medial to the inferior epigastric vessels. Which hernia is most likely being repaired?
- Direct
- Indirect
- Femoral
- Diaphragmatic
A lumbar plexus injury could result at which of the following spinal levels?
- L1-L4
- T11-L3
- L1-L3
- L2-L5
An 18-year-old male was riding his bike when he suddenly hit into a moving vehicle. Injuries were sustained at L1. The patient was then seen in your office complaining of numbness and abnormal sensation of the scrotum. Which nerve injury is the most likely culprit of his symptoms?
- ilioinguinal nerve
- Femoral nerve
- Posterior scrotal nerve
- Inguinal nerve
Which vein is most likely to be injured during a superficial laceration to the posterior aspect of the calf?
- Lesser Saphenous vein
- Femoral vein
- Epigastric vein
- Illiac vein
Author of lecture Posterior Compartment of Leg

Stuart Enoch, PhD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
