Playlist
Show Playlist
Hide Playlist
Physical Exam Findings of Cholecystitis and Appendicitis

-
Reference List Physical Examination.pdf
-
Download Lecture Overview
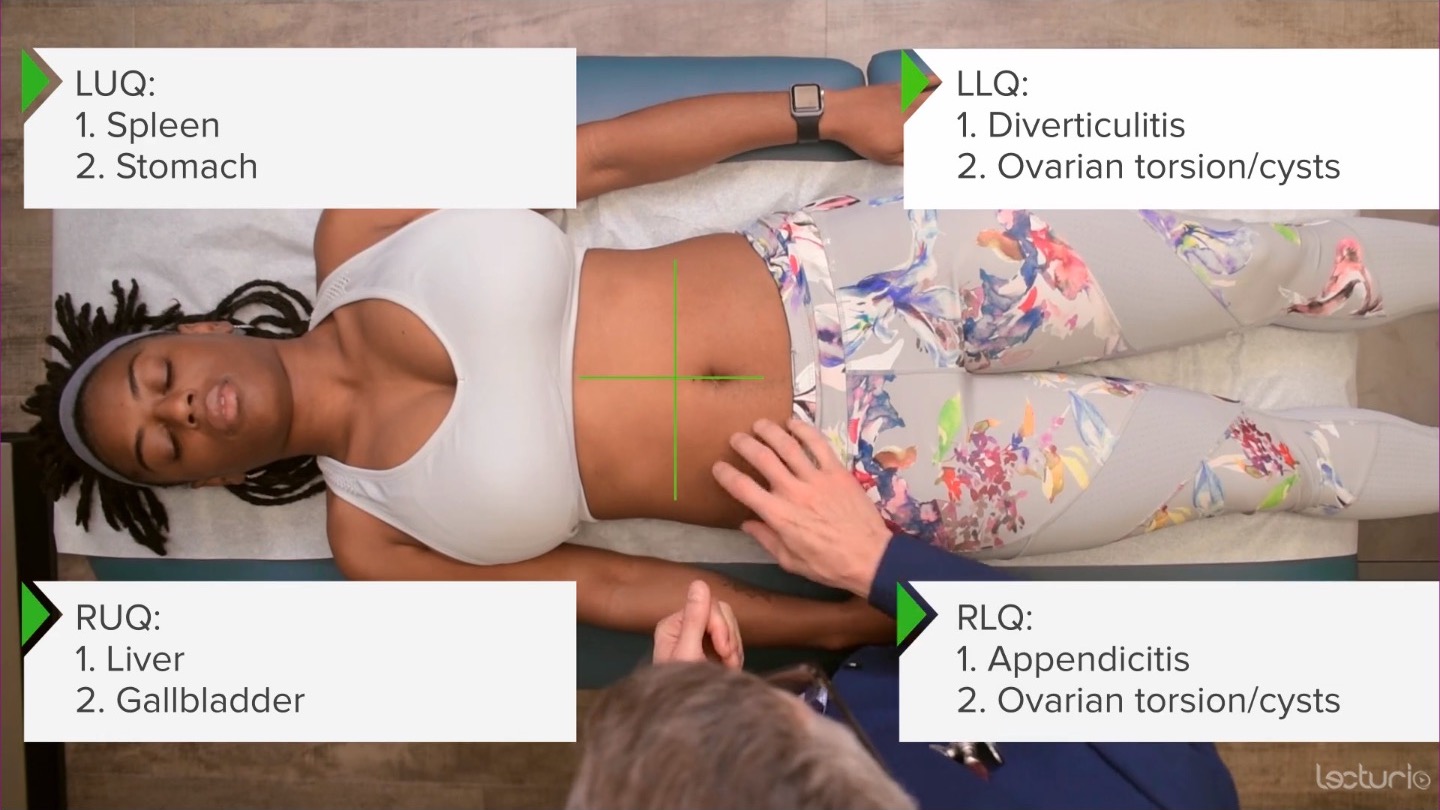
00:01 So, having talked about some of those specific disease pathologies, it's time to talk about the assessment of abdominal pain itself. 00:08 There are many patients who come in with abdominal pain and the trick with physical diagnosis is to determine whether this person has a benign cause of abdominal pain such as irritable bowel syndrome, or maybe even just constipation versus something intense, you know, something really severe like a perforated appendicitis, for example. 00:28 Patients with abdominal pain can again either have benign causes, abdominal wall pain that causes simply a painful tender organ, like an example of diverticulitis, and then a perforated viscous causing peritonitis. 00:43 The last, the latter of which, of course, is a surgical emergency, and is something we don't want to miss. 00:52 All patients may have tenderness on exam and all the circumstances that I just described, and all of them may have voluntary guarding, which is, you know, if there's a tender organ in there, the patient does not want me pushing on it. 01:03 So they're going to contract their abdominal wall muscles. 01:06 The astute clinician, however, can distinguish between voluntary guarding and involuntary rigidity. 01:14 So rigidity is when, there's so much inflammation in the belly and in the peritoneum, that it's causing reflex muscle spasm that the patient has no control over. 01:24 So, it's important for us to try and tease apart what's going on because obviously, with actual rigidity and acute abdomen, we need to get surgery involved. 01:32 So ways to do this are as follows. 01:34 Number one, as I said before, we would have her flexure hips a little bit just to relax the abdominal musculature. 01:39 But for the purposes of what we're doing now, I'll leave her legs down. 01:44 Next up, it's good to start palpating the abdomen, even before the patient knows you're palpating the abdomen. 01:50 And what I mean by that is, I'm going to have my stethoscope on back when I was auscultating, I'll be talking to my patient: Asking her about where she's from? Asking her what she does for a living? Talking to her, you know, telling jokes, asking her about her family, whatever. 02:06 And I've just done my palpation exam without her even knowing it. 02:10 Now, it sounds like I'm being disingenuous or slippery there, but it's important to distinguish between so called distractible tenderness, versus real intense tenderness, where even if I'm talking to her about something unrelated to why she's here today, if she feels every motion of my hand, and she's complaining of pain and asking me to stop, I know that's real tenderness. 02:33 And likewise, if her abdomen does not relax throughout that gentle prodding with my stethoscope, that tells me that rigidity real, real actual involuntary rigidity may be at play. 02:46 So, having said that, let's look at a few tests for specific types of painful pathologies in the abdomen, starting with acute cholecystitis. 02:54 Anyone who's had any degree of medical training knows about Murphy sign, and yet a lot of folks sometimes performing incorrectly. 03:03 So Murphy sign is based on the idea that the gallbladder is inflamed. 03:07 But when she is in exhalation, the diaphragm is higher and the liver, and the gallbladder are therefore higher up in the abdomen, and towards the thorax. 03:17 I'm going to put my fingers down in this area now. 03:19 And then I'm going to have the patient take a deep breath. 03:22 So take a deep breath for me. 03:24 Now, if while taking a deep breath, which again, her diaphragm is lowering the liver and the gallbladder towards my insulting fingers, if she abruptly stops taking that deep breath, that is the Murphy sign. 03:37 It basically is indication that by bringing her gallbladder slowly towards my fingers, if it arrests her breath, then it suggests the presence of acute cholecystitis. 03:50 Classically, you hear sonographic Murphy's, that's when the ultrasonographer is doing the exact same thing and has the patient take a deep breath, and that is also particularly a positive sign for acute cholecystitis. 04:02 Next up, for acute appendicitis. 04:04 There are many different signs that people have talked about for acute appendicitis and most noteworthy ones that have good data behind them is McBurney's point. 04:12 These are, basically there's a line drawn between the anterior superior iliac spine and the umbilicus. 04:19 And about two thirds of the way from the umbilicus to the anterior superior iliac spine is McBurney's point, which was hypothesized to be the place where you're most likely to detect appendicitis. 04:30 If a patient has point tenderness right in that spot that support the diagnosis of appendicitis. 04:36 Rovsing's sign is the idea that if I push on this side, and it causes pain over here, that also supports appendicitis, though somewhat less strongly. 04:44 And then the Psoas sign, named after the iliopsoas muscle is also helpful. 04:49 So, I'm going to have you roll over on your left hip now, please. 04:54 Since the appendix often lies just on top of the psoas muscle, if I can strain the psoas muscle where there may be some periappendiceal inflammation that could also support the diagnosis. 05:08 So, I'm simply going to take her leg and fully extend it. 05:11 So, I'm stretching her psoas muscle when I do this, and if that's elicits pain in that area around where McBurney's point was that would support the diagnosis of appendicitis as well. 05:21 You can lie back on your back now.
About the Lecture
The lecture Physical Exam Findings of Cholecystitis and Appendicitis by Stephen Holt, MD, MS is from the course Examination of the Abdominal Region.
Included Quiz Questions
A positive Murphy's sign is related to what clinical condition?
- Acute cholecystitis
- Acute diverticulitis
- Acute appendicitis
- Pelvic inflammatory disease
- Nephrolithiasis
A positive psoas sign is related to what clinical condition?
- Acute appendicitis
- Acute diverticulitis
- Pelvic inflammatory disease
- Nephrolithiasis
- Acute cholecystitis
Which of the following describes "guarding" in a patient with acute abdominal pain?
- The patient has contraction of the abdominal wall muscles to prevent increased pain on palpation.
- The patient is reluctant to discuss their pain.
- The patient appears defensive when asking them about their abdominal pain.
- The clinician observes relaxation of the abdomen upon palpation.
- The clinician observes pain relief upon abdominal percussion.
Author of lecture Physical Exam Findings of Cholecystitis and Appendicitis

Stephen Holt, MD, MS
Customer reviews
3,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
1 |
2 customer reviews without text
2 user review without text
