Playlist
Show Playlist
Hide Playlist
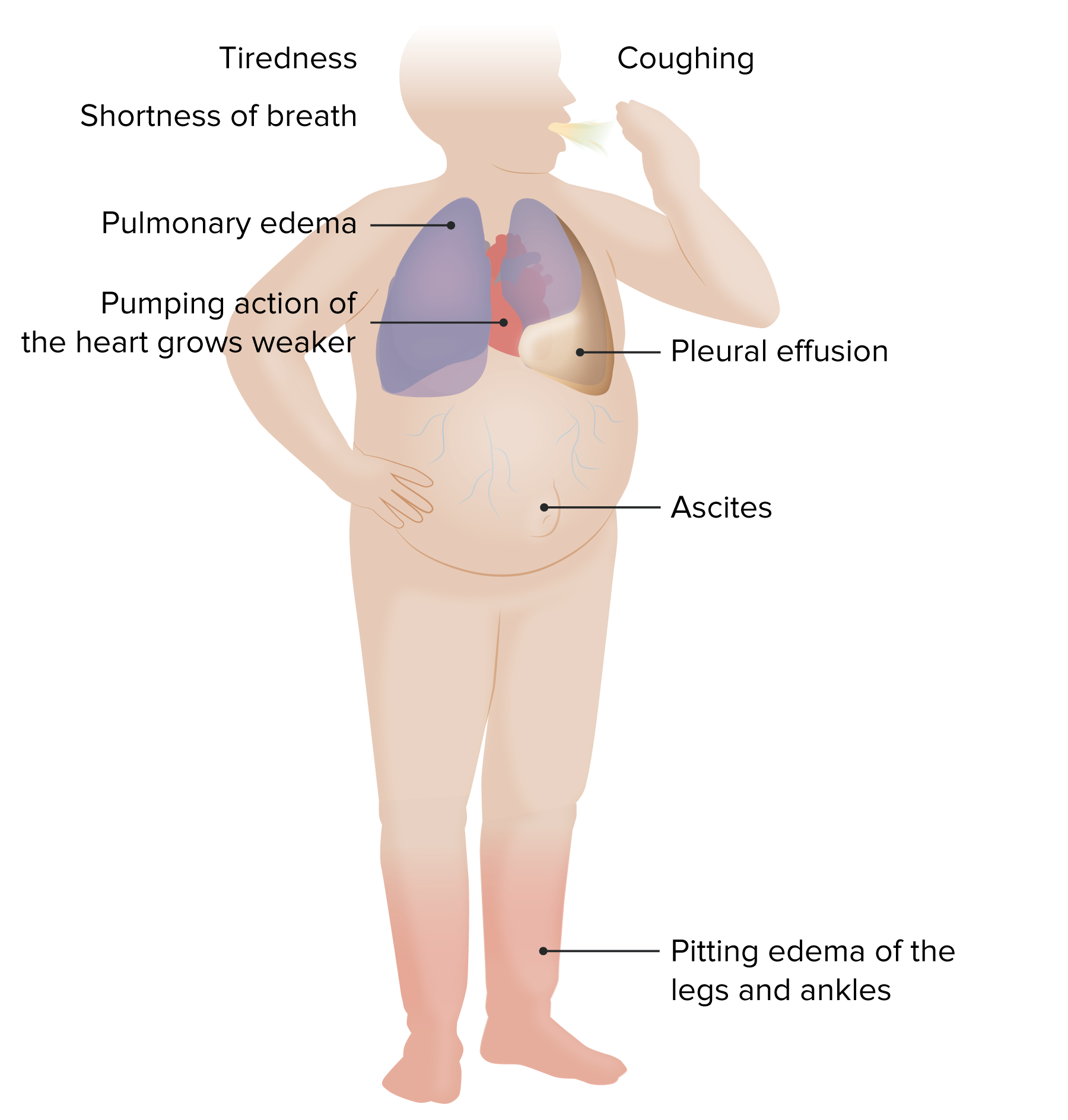
Peripheral Edema – Findings in Heart Failure


-
Reference List Physical Examination.pdf
-
Download Lecture Overview
00:01 Alright, so having talked about jugular vein distention and seeing how well that can help to identify acute congestive heart failure, we're also going to want to look for peripheral edema which can be an important sign as well. 00:12 So, let's take a look down here at the legs. 00:15 The most common place to find peripheral edema is going to be on your lower extremities, particularly in, if I may rotate the leg here, the pretibial areas in front of the shin, the shinbone, and down here in the pedal areas, so called pedal edema. 00:29 Assessing for edema is very simple, you're going to push on top of the skin, hold for two or three second and then quickly release and you're going to look and see if there's any pitting, that is if there is an indent left by your thumb after you pull your thumb away and typically, if it stays as a depression for a longer span of time, that may suggest more of a proteinaceous kind of edema like early lymphedema; or as if it resolves within five seconds or so, that may suggest more of a hydrostatic type of edema associated with heart failure or even an oncotic pressure type of edema for example from hypoalbuminemia or cirrhosis, etc. 01:10 The most common cause though of edema in the lower extremities is none of those very advance organ dysfunction problems, it's actually just chronic venous insufficiency which is a failure of the valves in the veins to return blood effectively to the heart, so all that is edema is not heart failure and that's why peripheral edema turns out to not be a particularly useful prognostic sign or diagnostic sign when you're trying to make a diagnosis of heart failure. 01:41 That being said, it's extremely useful when you're tracking a patient overtime as you're diuresing them for example. 01:48 In the same way they're tracking somebody's weight can be help when you're trying to see if you've diuresed them or over-diuresed them, etc. 01:55 So not useful to make a diagnosis but useful to track patients overtime. 01:59 Importantly, when you do push on the skin, you may find that a patient looks like the leg is swollen and edematous, but you push down and immediately when put your thumb off, the indent is gone and that can be suggested of lymphedema, advanced lymphedema. 02:17 When somebody has acquired lymphedema or secondary lymph edema that has been progressive for a long span of time, whether it's from a prior lymph node dissection perhaps in the upper extremity, or even folks who have chronic venous insufficiency for a long span of time can develop this lymphedematous process or secondary lymphedema or Verruca's lymphedema, you're going to find that the skin is so fibroused and thick that when you push, you can't push in very far and there's no indentation that's lefts afterwards so the interpretation of edema can be very nuance and it's important to realize that its useful, but it's not going to make or break a diagnosis of heart failure. 02:58 Since we're here in the legs though it's worth us taking a look at the pulses that you can identify in the legs. 03:05 We're going to talk more in a moment about the posterior tibial pulse, it's right here behind the medial malleolus, you can palpate it there. 03:12 The dorsalis pedis pulse is going to be located here, just a little bit lateral to the very prominent first MTP joint there. 03:22 Secondly, there is a popliteal pulse, very difficult to find for me at least, but its going to be found in the popliteal fossa between the semimembranosus and semitendinosus tendons on the left or the medial and lateral aspect of the back of the knee, and then the femoral artery is going to be up here. 03:43 Remember the N-A-V-L, the nervous system, the artery, the vein, and the lymphatics is how we can identify the different structures that are in the proximal thigh and the femoral artery could certainly by diseased, you may find a bruit there, etcetera, and the setting of peripheral arterial disease, but more often than not, you're going to find some disease farther down.
About the Lecture
The lecture Peripheral Edema – Findings in Heart Failure by Stephen Holt, MD, MS is from the course Examination of Cardiovascular and Respiratory System.
Included Quiz Questions
The physical exam finding of pitting edema in the ankles and feet is...
- ...seen with chronic venous insufficiency.
- ...a response to diuresis in heart failure.
- ...related to arterial pressure.
- ...due to hyperlipidemia.
- ...due to hypertension.
What is TRUE regarding the arterial pulses in the lower extremities?
- The posterior tibial pulse is located behind the medial malleolus of the ankle.
- The dorsalis pedis pulse is located behind the medial malleolus of the ankle.
- The posterior tibial pulse is located on top of the foot lateral to the first metatarsophalangeal (MTP) joint.
- The popliteal pulse is located on top of the foot lateral to the first MTP joint.
- The femoral pulse is located behind the knee.
Author of lecture Peripheral Edema – Findings in Heart Failure

Stephen Holt, MD, MS
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
