Playlist
Show Playlist
Hide Playlist
Pediatric Pulmonary Embolism (PE)

-
Slides Pulmonary diseases in older children.pdf
-
Download Lecture Overview
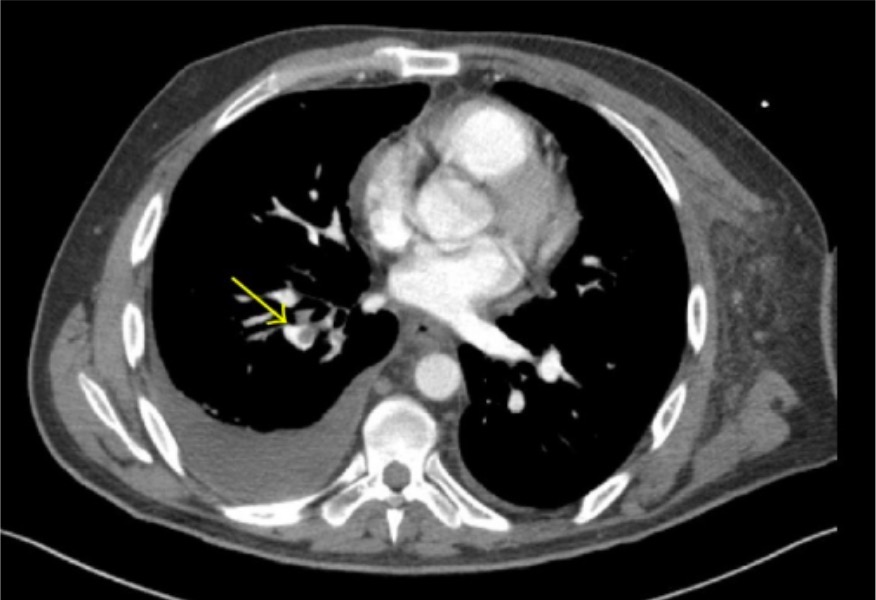
00:01 In this lecture we're going to discuss pulmonary diseases that show up in older children. Now we're going to exclude cystic fibrosis which has its own lecture. And we're excluding pulmonary diseases that show up in infants, which also has its own lecture. 00:18 This is really other problems in children. 00:22 Let's start off with pulmonary embolism. 00:26 So a pulmonary embolism can happen. 00:30 And it's but it's very rare in children compared to adults. 00:34 It is seen more commonly in diseases or circumstances where there's a predisposition to forming a clot. 00:43 And the mortality rate is only 20% that of adults. 00:48 In other words, children's are more likely to have smaller pulmonary embolisms, and they're more likely to survive the event and live past it. 00:59 So in order to understand the pathophysiology of the pulmonary embolism, we have to recall Virchow's triad the three things that are resulting in a clot inside a blood vessel. 01:11 One is stasis, one is the hypercoagulable state and the other is endothelial damage. And if we have these three things, we're at increased risk for creating a thrombus inside the child. 01:25 That thrombus can then proceed up and into the lungs where it causes the pulmonary embolism. 01:32 One way to remember it is eyes and nose. 01:35 So there are I's and O's that are responsible for causing pulmonary embolism. 01:40 The eyes are indwelling central lines. 01:44 Prolonged immobilization or inherited disorders of coagulation. Remember in kids they present with unusual congenital problems more often than adults do. 01:56 So these inherited disorders are something we will absolutely think of in a child who presents with a pulmonary embolism. 02:05 The OHS, obesity oral contraceptive pills or orthopedic surgery which is really more of the immobilization, but a nice way to remember that. 02:17 So in terms of the pathology of the disease, most pulmonary embolisms start as a thrombus in a vein and then fly into the lungs. 02:27 This is usually starting off in a lower extremity, but can be in the upper extremity or the pelvis, the kidney, or the even just the right side of the heart. 02:36 And as we stated before, these are rare. 02:38 But even rarer still are air emboli, tumor emboli or fat emboli, which can cause similar symptoms but aren't necessarily from a clot. So the pulmonary embolus, if it's rare, how do we suspect it? These patients will typically have a history of sudden onset pleuritic chest pain. They'll have difficulty of breathing that is sudden onset. 03:07 About 50% of them will have a cough and about a third of them will have hemoptysis. Hemoptysis in a child is never normal if they're presenting with a massive pulmonary embolism, which is exceptionally rare and much rarer than in adults. 03:25 These patients will have a sudden onset cyanosis and right ventricular failure. These are the patients with jugular venous venous distention hepatomegaly. 03:37 They may have a single loud S2. 03:40 Other problems like that. 03:43 The majority of children presenting with a pulmonary embolism though are going to be non-massive. Ps about half of these children will have tachypnea. 03:52 They will often have tachycardia, and you may auscultate while you're examining them. You may hear crackles, wheezing, or usually they're just clear to auscultation. So as you can see a lot of these symptoms are somewhat nonspecific. 04:10 And in children it's a rare condition. 04:13 So you can imagine this is a challenging diagnosis to make. 04:16 And it is while we always keep radiation exposure in mind for children. 04:21 Ct pulmonary angiography remains our imaging modality of choice for diagnosing PE in pediatrics. 04:29 Unlike adults, commonly used decision tools, including the Wells score and D-dimer, have not been shown to reliably discriminate between children with and without PE. So we don't use them to rule in or rule out disease. Alternative imaging can be helpful when ctpa is contraindicated, unavailable, or inconclusive. 04:52 A v, q scan or Mr. pulmonary angiography avoids ionizing radiation, but these studies are typically slower and often require sedation in young children. 05:04 Echocardiography plays a supporting role. 05:07 It may show right ventricular strain, which carries prognostic value, but echo alone is insensitive or specific. 05:16 Many patients with PE have a normal study, and RV strain can occur from other causes. Among other tests, an ABG may show decreased pao2 reflecting v q mismatch from the clot, and a chest x ray may show an area of collapse. 05:34 These are nonspecific, but they can support the overall assessment.
About the Lecture
The lecture Pediatric Pulmonary Embolism (PE) by Brian Alverson, MD is from the course Pediatric Pulmonology.
Included Quiz Questions
Which test is most likely to rule out a pulmonary embolism in a pediatric patient?
- A normal D-dimer
- A normal arterial blood gas
- A normal chest x-ray
- A normal basic metabolic panel/CHEM-7
- A normal venous blood gas
A 16-year-old female comes to you with shortness of breath and chest pain. You suspect pulmonary embolism and proceed with necessary lab tests. Which of the following is a highly unlikely cause of pulmonary embolism?
- Isotretinoin
- Recent Immobilization
- Inherited coagulation disorder
- Obesity
- Oral contraceptive pills
Which of the following tests is used to rule in pulmonary embolism in a pediatric patient?
- Spiral CT
- ESR
- MRI chest
- Chest X-ray
- Arterial Blood Gases
Author of lecture Pediatric Pulmonary Embolism (PE)

Brian Alverson, MD
Customer reviews
4,0 of 5 stars
| 5 Stars |
|
0 |
| 4 Stars |
|
1 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Very good lecture. This allowed me to transfer my knowledge from the adult medicine to pediatrics regarding PE. However, I would have liked more info regarding the link with DVT and the clinical aspects of PE in children like clinical cases maybe and also a part about management. That being said I do understand it is not a typical pediatrics disease as it can be in adult medicine.
