Playlist
Show Playlist
Hide Playlist
Pediatric Meckel’s Diverticulum

-
Slides Appendicitis and Meckel's Diverticulum Pediatrics.pdf
-
Download Lecture Overview
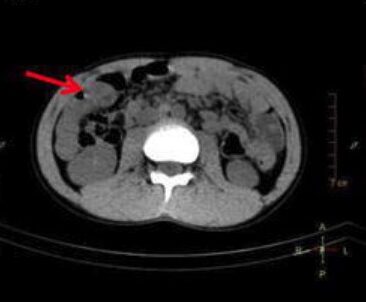
00:02 Let’s shift gears a little bit and talk about another type of presentation. 00:06 Here’s a five-year-old girl who’s coming into the emergency department with bloody and occasionally melanotic stools. 00:12 Lab works shows that she’s got a little bit of an iron deficiency anemia. 00:17 She denies pain. 00:19 And according to mom, other than strange stools, she’s been relatively asymptomatic. 00:26 We like to think of the appendix as an outpouching of intestinal material around the cecum. 00:33 And in this case, this is another one that happens in only a smaller percentage of the population. 00:38 So this is going to be a Meckel’s diverticulum. 00:44 The Meckel’s diverticulum is a failed involution of the vitelline duct. 00:50 As you can see on the slide here, it’s generally an outpouching, a diverticulum, of the intestine that’s heading up towards the umbilicus. 01:01 This is the most common true diverticulum in humans. 01:05 And it’s the common congenital malformation of the GI tract. 01:13 So an important rule to remember is the rule of twos. 01:17 This is highly likely to show up on a multiple choice exam. 01:23 So Meckel’s diverticulums occur in 2% of the population. 01:29 They are two times as common in males than they are as females. 01:34 They are generally 2 inches long. 01:37 They generally occur 2 feet before the ileocecal valve. 01:43 And so if you can remember those rules of twos, you’ll be in good shape on the exam that you’re going to take. 01:50 Generally, these patients will present with bleeding from their Meckel’s and we’ll talk about why in a second. 01:56 But you’ll see that they’ll have melanotic or black stools. 02:00 They may have bloody stools or rectal bleeding. 02:04 But in general, they’ll be asymptomatic, they won’t have pain from this. 02:08 It will just be a brisk GI bleed. 02:12 Occasionally, they can develop bowel obstruction and occasionally, they may get some anemia as well. 02:19 Generally, it’s a slow bleed. 02:21 So they may have an iron deficiency anemia from simply not replacing their body iron stores as they’re making new blood to replace the old blood. 02:31 The bowel obstruction may be from something called an intussusception and we’ll learn about that in another talk but keep that in mind. 02:41 The way we test for a Meckel’s diverticulum is by using a radionucleotide scan, a technetium-99m pertechnetate scan. 02:53 And we’re going to look for gastric mucosa that is outside the stomach. 03:00 So you can see here that mucus cells have taken up the pertechnetate and they’ve done it as where the arrow shows on this slide at the level of a Meckel’s, which is outside the stomach, which is the large dark blob that you can see at the top of the slide. 03:19 70% of cases of a Meckel’s will be found this way. 03:25 But that means that 30% of cases of Meckel’s will not. 03:30 So if we suspected a Meckel’s that will not, we’ll look for other imaging modalities like ultrasound, MRI, and CAT scan like we did in the appendicitis. 03:41 How do we treat a Meckel’s? Simply just like we did in appendicitis, this requires a surgical excision. 03:51 So in summary, those are two common problems in children which are outpouchings or diverticuli of the intestinal wall that can cause problems in children. 04:03 Meckel’s is a painless bleed whereas the appendicitis is an acute infection. 04:08 Thanks for your attention.
About the Lecture
The lecture Pediatric Meckel’s Diverticulum by Brian Alverson, MD is from the course Pediatric Gastroenterology.
Included Quiz Questions
Which of the following is NOT true about a typical Meckel’s diverticulum?
- They present with 2 days of symptoms
- They affect 2% of the population
- They are twice as common in males
- They are 2 inches long
- They are 2 feet proximal to the ileocecal valve
Which of the following is the investigation of choice for the diagnosis of Meckel's diverticulum?
- Technetium-99m pertechnetate scan
- Ultrasonogram of abdomen
- CT abdomen
- MRI abdomen
- Plain x-ray abdomen
Author of lecture Pediatric Meckel’s Diverticulum

Brian Alverson, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Great lecture! Concise, informative, clear. Perfect lecture for a resident in the emergency hospital setting.
