Playlist
Show Playlist
Hide Playlist
Pediatric Glomerulonephritis


-
Slides HematuriaGlomerulonephritis Pediatrics.pdf
-
Download Lecture Overview
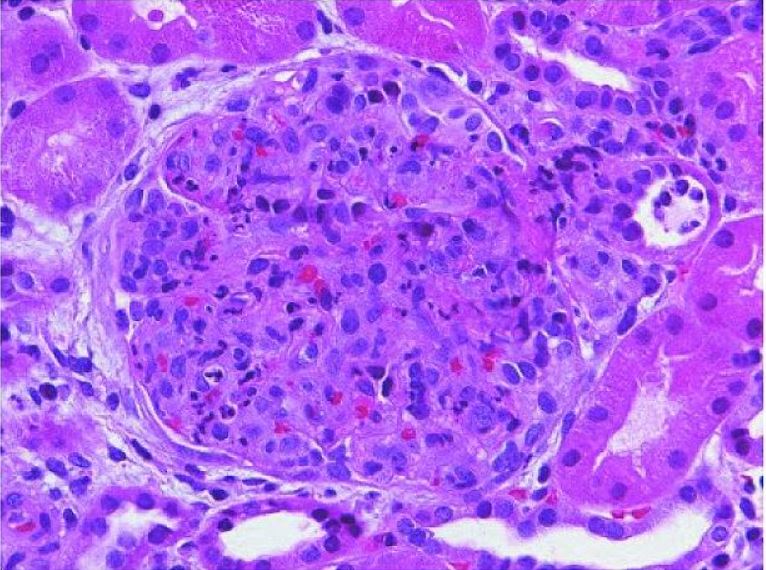
00:01 So let’s focus on what’s happening when we have an abnormal glomerulus and in particular, inflammation of the glomerulus which is glomerulonephritis. 00:11 As you recall from your histopathology, here’s a normal glomerulus and here’s an abnormal glomerulus and you can see it is heavily infiltrated with white blood cells and inflammatory cells. 00:23 So the inflammation of the glomerulus has many potential causes and it can in turn result in hematuria and proteinuria, red blood cell casts and that’s a great way to distinguish between glomerulonephritis and cystitis. 00:41 And sometimes can result in hypertension through abnormal renin secretion or even frank renal failure. 00:50 So glomerulonephritis which is blood and protein coming out, spilling out of the urine through that abnormal glomerulus can be broken down into a few categories. 01:03 It can be acute that usually has red blood cell casts and that acute glomerulonephritis maybe either primary, something wrong with the kidney, or secondary, something wrong systemically. 01:16 Alternatively, glomerulonephritis maybe chronic. 01:19 And in this case often, they are not red blood cell casts and with chronic disease, again this can be either primary or secondary. 01:29 So I want to go through examples of diseases that are either acute, primary and secondary or chronic, primary and secondary. 01:37 So let’s start with acute glomerulonephritis. 01:41 This is the one which often presents with red blood casts. 01:45 We have primary and secondary causes. 01:48 The primary causes include commonly post-strep glomerulonephritis. 01:53 Remember, that treatment of strep throat does not prevent post-strep glomerulonephritis like it does rheumatic fever. 02:01 It could be an infectious glomerulonephritis, basically a pyelonephritis, or it could be IgA nephropathy which is also called Berger’s disease. 02:11 Or it could be membranoproliferative glomerulonephritis or MPGN. 02:16 Secondary causes of acute glomerulonephritis are systemic problems that will acutely cause the kidneys to bleed. 02:26 The most common is Henoch-Schonlein purpura. 02:29 Also, lupus can do it or patients may have polyarteritis nodosa which is a systemic disease that can involve the kidneys. 02:38 Patients may have hemolytic uremic syndrome which absolutely causes renal damage. 02:43 This is what you got after getting bad strains of E. coli. 02:47 Patients may have subacute endocarditis which is flicking little clots which is damaging the kidney and causing acute bleeding. 02:55 Or patients may have something like Goodpasture syndrome which is an inflammation of the basement membrane in the kidney. 03:01 Chronic glomerulonephritis may result in significant bleeding. 03:08 This is an ongoing issue. 03:10 These patients typically don’t have casts and the primary causes include again membranoproliferative glomerulonephritis. 03:19 Patients may have membranous nephropathy. 03:22 They could have focal glomerulosclerosis or they may have mesangial proliferative nephritis. 03:28 Those are all chronic conditions that can cause a primary glomerulonephritis and a primary bleeding in the urine. 03:36 The secondary causes of chronic are the same as the first. 03:40 HSP may become chronic in those unfortunate patients who end up with longstanding renal disease, obviously lupus, polyarteritis nodosa, HUS, subacute endocarditis and Goodpasture syndrome. 03:53 This can all be chronic conditions. 03:55 So the diagnosis of glomerulonephritis, if you suspect it, is not always made by a biopsy. 04:03 We do not require biopsy in patients where there is clear explanation for the disease. 04:08 Examples would be post-strep glomerulonephritis where we knew the child had strep throat two weeks ago or the very obvious situational conditions of hemolytic uremic syndrome and Henoch-Schonlein purpura. 04:22 If you want to know more about these diseases, there are separate lectures on those. 04:26 We generally, for those diseases, target therapy towards the underlying problem as opposed to the kidneys. 04:34 We can check C3 and C4 levels and that can help us distinguish between some causes of glomerulonephritis. 04:43 This is important. 04:45 We typically see low C3 and normal C4 in post-strep glomerulonephritis. 04:53 However, we see low C3 and low C4 in lupus, shunt nephritis and bacterial endocarditis. 05:03 So lupus has a low C3 and low C4 and post-strep glomerulonephritis just a low C3. 05:12 So for those patients where you think it’s post-strep glomerulonephritis, you got a low C3 and a normal C4, that child probably does not require a biopsy. 05:22 The prognosis for glomerulonephritis in general is excellent. 05:28 Some of the diseases end up chronic but that’s the vast minority. 05:32 So 98% of children will make a full recovery whereas 2% will go on to have chronic renal failure or some form of chronic kidney disease. 05:42 That’s a summary of hematuria and glomerulonephritis. 05:46 Thanks for your attention.
About the Lecture
The lecture Pediatric Glomerulonephritis by Brian Alverson, MD is from the course Pediatric Nephrology and Urology. It contains the following chapters:
- Glomerulonephritis
- Acute Glomerulonephritis
- Chronic Glomerulonephritis
Included Quiz Questions
A patient has a low C3 but a normal C4. What is the most likely cause of their hematuria?
- Poststreptococcal glomerulonephritis (PSGN)
- Pyelonephritis
- IgA nephropathy
- Lupus nephritis
- Membranoproliferative glomerulonephritis (MPGN)
Which of the following conditions is typically considered a systemic disorder that causes secondary glomerulonephritis?
- Henoch-Schonlein purpura
- IgA nephropathy
- Minimal change disease
- Membranoproliferative glomerulonephritis
- Membranous nephropathy
Which of the following conditions typically requires a renal biopsy for diagnosis?
- Focal segmental glomerulosclerosis
- Poststreptococcal glomerulonephritis
- Henoch-Schonlein purpura
- Hemolytic uremic syndrome
A 14-year-old presents because of an erythematous rash over the nose and cheeks. She also complains of skin rash over the face and hands following exposure to sunlight. She has bilateral joint pain and swelling in her hands and knees. Urine examination shows hematuria and proteinuria. Serological testing shows low C3 and C4 with a positive antinuclear antibody test. Which of the following is the most likely diagnosis in this patient?
- Systemic lupus erythematosus
- Poststreptococcal glomerulonephritis
- Hemolytic uremic syndrome
- Henoch-Schonlein purpura
- IgA nephritis
Author of lecture Pediatric Glomerulonephritis

Brian Alverson, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Excellent lecture. Nephrology is a topic that is often obscured by the teachers in this field I met. This is not the case in this lecture. Let there be light ;)
