Playlist
Show Playlist
Hide Playlist
Pathology of Alzheimer's Disease

-
Slides 02 AnomaliesAgingBrainAlzeheimerDementia Aging.pdf
-
Download Lecture Overview
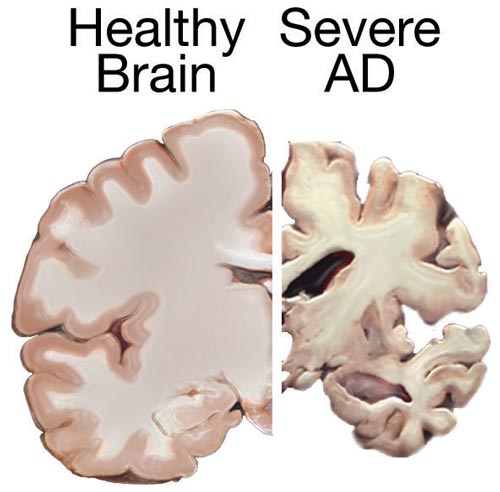
00:01 Before we go there, let’s look at these plaques and tangles. First of all, we could have development of plaques. Those plaques happen, the beta amyloid plaques happen between different neurons, so outside of the neuron between neurons and perhaps interrupt signaling. The second component are these neurofibrillary tangles which occur inside the neurons and block the passage of signaling molecules and nutrients to and from the nucleus. Let’s take a closer look at the beta amyloid plaques. 00:41 We’ll deal with those first to look at where they are derived from. We can see in the first figure here there is what we call amyloid precursor protein. It’s a normal protein in the cell membrane. 00:55 For some reason, it gets clipped and released. These pieces of beta amyloid are released. 01:05 The beta amyloid piece of this protein that’s released is particularly sticky. So, it will associate with other pieces that are sticky and cause a beta amyloid plaque, so association of different pieces of the same kind of protein. These occur between neurons, again outside of the cell. 01:28 They interrupt communication between cells especially at the synapses. When the cells stop communicating with each other, they stop getting signals that’s worth living on. So, the immune response comes in and starts clearing those cells. So, we see degeneration of those neurons. 01:49 The cells actually undergo apoptosis and are removed which is why we see a decrease in brain size. 01:57 I’ll show you an image of that shortly. The second component where these neurofibrillary tangles, if you can say that mouthful in front of a camera, good on you, neurofibrillary tangles result from abnormalities in proteins within the cell. First of all, recall that there are microtubules inside of every cell. 02:21 They’re part of the cytoskeletal network. Microtubules in particular are about transporting things around in the cells. This pink and yellow molecule here is a microtubule. It may extend the length of a whole neuron as we transport things from the nucleus, perhaps neurotransmitters and such, all the way down to the signaling end or to the extreme regions of the cell. These rails, so to speak are held stably in line. Let’s imagine they’re railroad tracks. Perhaps, we need to spike them down so that they don’t move when the trains come by. They are stabilized by a protein called tau. 03:08 So, the tau protein in Alzheimer's comes out in a mutated form or begins to become mutated. 03:16 So, the tau protein no longer acts to stake down the tracks which then disrupts the continuity of the tracks so that these molecular motors and transport proteins can’t run along them anymore. 03:32 These tangles prevent passageway of all the nutrients and goods along the length of the neuron. 03:42 Consequently, the neuron is not signaling in the way that it should and it will be degraded. 03:49 That is what leads us to the development of reduced brain size at the end of the progression of Alzheimer's disease. Again, I mentioned there’s a characteristic spread of Alzheimer's. 04:04 As we watch Alzheimer's progress in individuals, we first see that learning and memory is lost. 04:12 We see excessive loss of learning and memory associated with damage in the anterior temporal lobe. 04:20 Then it will generally progress towards degeneration in thinking and planning future events. 04:29 That is a consequence of damage that we see in the frontal lobe. Then it moves more to the posterior region of the temporal lobe and starts affecting speech and communication. As the disease progresses, you can see the development of the beta amyloid plaques and neurofibrillary tangles progress throughout the brain. As it spreads to other regions, for example the parietal lobe, individuals start losing their sense of location and their surrounding environment. Again, this is a fairly characteristic spread of Alzheimer's disease. It’s not exactly the way it happens all the time. So, you may witness different progressions in different individuals. Here is a great image showing the sort of scope of neuronal death, right? A regular brain on the left-hand side and over on the right-hand side, we see a brain that has been affected by Alzheimer's. There’s much reduced mater shrinkage in the cerebral cortex as well as expanded ventricle. This is not really a good outcome but there’s serious evidence of actual degradation of neurons, right? They’ve been destroyed because of the beta amyloid plaques or the neurofibrillary tangles and a combination of both. 06:01 How do we treat Alzheimer's disease? One of the things that we think about in communication between neurons, if you were to name a neurotransmitter that you know exists in the brain, what would it be? Right, acetylcholine. Acetylcholine where we see reduction of the number of neurons and thus the reduction of signaling between neurons and the reduction of acetylcholine. 06:29 So, that’s one of the characteristics or one of the features that ends up in Alzheimer’s displaying the way it does. One of the most frequent treatments is the use of cholinesterase inhibitors. 06:43 The idea here is that we prevent the destruction of acetylcholine so that it remains present in the synapse for longer and has more potential to signal the neuron downstream. It’s fairly effective at treating Alzheimer's for a certain amount of time. Of course, the disease is progressive so eventually, we’re going to go down the path of degeneration anyway. A fairly new advent, although a not new drug is the use of a drug called memantine sold under the name of Namenda, which actually has been around for quite some time since the late 60s. It was initially made to treat diabetes. It turns out that it’s fairly effective at treating later stages of Alzheimer's disease also. So, what it does is antagonizes that NMDA receptor to block glutamate receptors. So, we see that glutamate doesn’t have as much of an effect. It’s suggested that the reason that it does this is in some Alzheimer's patients, we may see an excess of glutamate which overstimulates. When a glutamate is there overstimulating receptors then we see loss in memory and disassociation there. So, by blocking the NMDA receptors, we decrease the action of glutamate and thus decrease the progression of the disease. So, a drug that’s been around for a long time that has resurfaced as a potential treatment. It’s fairly successful in later stages of Alzheimer's although not as successful in the earlier stages where we’re just seeing increased forgetfulness. 08:39 Monoclonal antibodies directed against beta amyloid have recently been approved for individuals with Alzheimer disease a and mild cognitive impairment. 08:49 These include aducanumab and lecanemab. 08:53 While these medications do appear to reduce beta amyloid plaques on the brain, whether this correlates to clinical improvement remains to be seen. 09:02 Additionally, MRI monitoring is required to evaluate for amyloid-related imaging abnormalities, such as edema, hemosiderin deposition, and microhemorrhages.”
About the Lecture
The lecture Pathology of Alzheimer's Disease by Georgina Cornwall, PhD is from the course Aging.
Included Quiz Questions
Which of the following statements about the pathology of Alzheimer's is true?
- Beta-amyloid plaques build up in the synaptic region between neurons and block inter-neuronal signaling.
- Beta-amyloid plaques build up inside neurons and block the passage of neurotransmitters from the nucleus to the synapse.
- Tao protein tangles build up in the synaptic region between neurons and block inter-neuronal signaling.
- Beta-amyloid plaques interrupt the integrity of microtubules in a neuron.
- Tao protein plaques attach to neurotransmitters and block synaptic communication between neurons.
Which of the following best describes beta-amyloid plaques?
- They are an accumulation of parts of clipped cell membrane proteins that build up between neurons, blocking communication at the synapse.
- They are mutated proteins inside a neuron.
- They clog up normal transport via microtubules in a neuron.
- They are formed by an immune response that destroys cells.
- They are direct antagonists of neurotransmitters and block their effect at the synapse.
Which of the following does NOT describe the typical pathology of Alzheimer's disease?
- Alzheimer's disease usually first manifests as a decline in a patient's ability to communicate.
- The accumulation of neurofibrillary tangles inside neurons blocks the passage of neurotransmitters from the nucleus to the synaptic region of a neuron.
- The accumulation of beta-amyloid plaques between neurons interrupts neurotransmitter signals at the synapse.
- The body's immune response initiates apoptosis of neurons that are unable to communicate causing brain atrophy.
- Alzheimer's is a neurodegenerative disorder.
Which symptoms are associated with Alzheimer's disease when it affects the anterior temporal lobe?
- Learning disability and memory loss
- Loss of capacity for complex thinking and future planning
- Loss of sense and awareness of the surrounding environment
- Difficulties with speech and communication
- Change in personality and emotional behavior
How do cholinesterase inhibitors work to treat Alzheimer's disease?
- They increase the amount of time acetylcholine remains at the synapse, increasing its potential for neuronal communication.
- They decrease the amount of time acetylcholine remains at the synapse, increasing its potential for neuronal communication.
- They act as an antagonist against glutamate receptors on the postsynaptic neuron.
- They act to dissolve amyloid plaques in the synapse.
- They act to stabilize microtubules for improved transport of neurotransmitters.
Author of lecture Pathology of Alzheimer's Disease

Georgina Cornwall, PhD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
2 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
I liked his explanation: first the context and then see the Alzheimer's itself.
Excellent lecture. Loved that it was succinct and to the point.
