Playlist
Show Playlist
Hide Playlist
Osteogenesis Imperfecta (Brittle Bone Disease) in Children

-
Slides OI Pediatrics.pdf
-
Download Lecture Overview
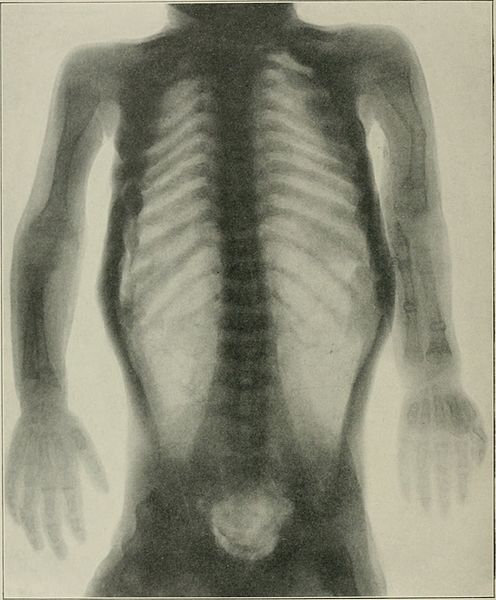
00:01 In this lecture, we’re going to discuss osteogenesis imperfecta. So, osteogenesis imperfecta is a spectrum of different diseases but they all have one thing in common, severe bone fragility. All of these diseases are caused by mutations in the gene that codes for type 1 collagen. It’s mostly autosomal dominant or new mutations, although there are some rarer subtypes that are autosomal recessive. 00:34 Basically, the bone has decreased trabeculae. This results in reduced cortical thickness and increase in osteoblast and osteoclast activity. So, fractures are more frequent. These children will get fractures from just simple movement. Healing occurs normally. So, there are four major types of osteogenesis imperfecta. 01:00 Many of them can have abnormalities in what we call dentinogenesis imperfecta. Dentinogenesis is when the teeth are involved too. The teeth will be bluish greyish and will be more fragile. For type III, dentinogenesis imperfecta is known to happen. For types I and IV, they’re broken down into subtypes A and B. 01:27 So, type IA and IVA do not have dentinogenesis and types IB and IVB do. Type II is often fatal, so we don’t see that so often in children. Type IV has frequent long bone deformities at a baseline as well. 01:47 So, let’s review a little bit more about how children appear when they show up with osteogenesis imperfecta. 01:56 Here is such a patient. You’ll notice this child has multiple broken bones throughout his body. 02:03 This is not because of child abuse. This is simply from base lying handling of this child. Another finding that you see in many subtypes of osteogenesis imperfecta is blue sclera. You can see this child's sclera are slightly blue tinged. That happens quite frequently in osteogenesis imperfecta but can also happen in other connective tissue disorders such as Marfan or Ehlers–Danlos. One thing about children with osteogenesis imperfecta is they may have hypercalciuria but it usually does not involve renal failure. 02:39 When we see these patients, we need to distinguish them from child abuse. On the flip side, and this is somewhat interesting, in patients who have suffered child abuse and have multiple fractures, we sometimes will test for osteogenesis imperfecta not because we actually suspect they have the disease but because we’re concerned that the defense may make an argument in court that we have not ruled out osteogenesis imperfecta as we’re trying to find a safe place for this child to be raised. The way we make the diagnosis is by DNA mutation analysis and prenatal diagnosis through amniocentesis is absolutely possible. So, treatment of osteogenesis imperfecta is largely through bisphosphonates such as pamidronate. This reduces fractures, increases bone density, and can also reduce pain. 03:35 It’s important to provide these children adequate vitamin D and calcium. Remember, their osteoblasts and osteoclasts are acting normally. If there’s increased turnover from bone injury, we need to make sure they are complete with these vitamins and minerals. Lastly, genetic counseling is important to families who have a child with osteogenesis imperfecta. Also, orthopedist should be involved and consulted routinely for fractures. It’s typical for us to ask a pediatric orthopedist to follow these children as they are complicated. 04:09 Adequate care is required by someone who is very familiar with this condition. The same can be said for physical therapist and occupational therapist. They have to know exactly how far it is safe to push these children and not cause fractures as a result of the important care that they provide. 04:26 That’s a summary of osteogenesis imperfecta. Thanks for your time.
About the Lecture
The lecture Osteogenesis Imperfecta (Brittle Bone Disease) in Children by Brian Alverson, MD is from the course Pediatric Rheumatology and Orthopedics.
Included Quiz Questions
Which of the following drugs is indicated in children with osteogenesis imperfecta?
- Pamidronate
- Etomidate
- Ranitidine
- Steroids
- Vitamin B6
Author of lecture Osteogenesis Imperfecta (Brittle Bone Disease) in Children

Brian Alverson, MD
Customer reviews
4,5 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
1 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Excellent lecture on this rare disease: not too much not too little. Also it's great that some societal context was given.
Simple straight forward info on Osteogenesis imperfecta. The medicolegal aspect is just well explained
