Playlist
Show Playlist
Hide Playlist
Neuroepithelial Tumors: Oligodendroglioma

-
Slides 08 Tumors of the CNS Neuropathology II.pdf
-
Download Lecture Overview
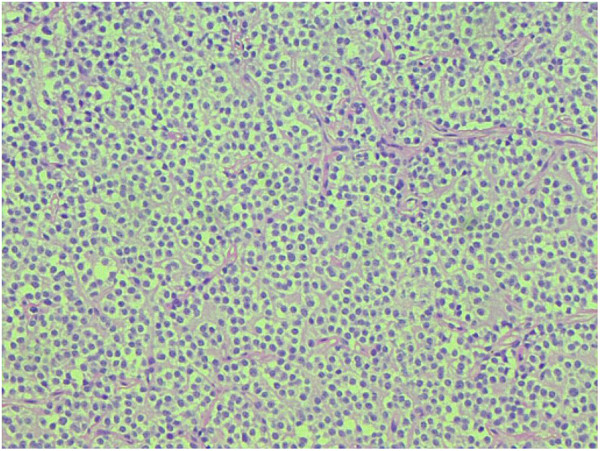
00:01 We now move on to another neuroepithelial tumor and you want to move away from astrocytoma. 00:07 We have now completed our discussion of astrocytoma officially. 00:12 And now we move on to these myelin production cells. 00:17 Well, originally. 00:19 But now, these myelin production cells of the CNS has now become a neoplasia, a primary brain tumor. 00:28 Welcome to oligodendroglioma, okay? So keep your astrocytes separate from your oligodendrocytes. 00:36 This is the most common in fourth and fifth decades. 00:40 Patients often have several years of neurologic complaints including seizures prior to diagnosis and found predominantly in the cerebral hemisphere specially in the white matter. 00:51 Now, these are an introduction to your oligodendrogliomas. 00:55 What else might you be looking for? Pathology: Well-circumscribed, gelatinous, gray masses often with cysts. 01:03 Remember, these are not referring to astrocytes. 01:06 And oftentimes, you’ll find calcification. 01:10 The sheets of the regular cells, this is important. 01:14 Please pay attention to spherical nuclei containing finely granular chromatin surrounded by a clear halo. 01:23 Picture that for me. 01:25 So you have the nuclei, which is perfectly circular. 01:27 In fact, I want you pick up an egg for me. 01:31 Crack it. 01:33 I have about a dozen eggs a day on average. 01:37 I do. 01:38 And every time I crack an egg, I always think of oligodendroglioma as you should as well. 01:44 When you crack an egg and you placed it properly in the pan, the yolk is perfectly spherical, huh? And then around that nucleus, that's spherical, you have that white halo. 01:56 That’s what you’re thinking about here with oligodendroglioma, very specific for this condition. 02:04 It usually contains a delicate network of anastomosing capillaries, that is another huge point. 02:10 Pay attention to lots of angiogenesis and resulting in capillary formation. 02:17 Obviously, with any type of neoplasia, you’re going to find increased angiogenesis, but the combination of a fried egg and the evidence of angiogenesis, no doubt, this is oligodendroglioma. 02:33 I like saying this word. 02:34 It’s actually really fun. 02:35 I don’t know what it is, but it brings me satisfaction to the brain. 02:38 Oligodendroglioma. 02:40 Anyhow, clinical features, average survival, five to ten years and more chemoresponsive than astrocytomas. 02:49 Do you understand that statement? Astrocytomas, quickly run through the ones that we’ve talked about or the ones you should know. 02:57 What you want to do is keep your adult astrocytoma separate from your child astrocytoma, right? So therefore, keep your pilocytic separate from the rest including your fibrillary, anaplastic, and glioblastoma. 03:11 Here, chemotherapy, well, could benefit a patient with oligodendroglioma. 03:18 If you take a look at this picture, what do we find? Fried eggs and bacon or sausage. 03:24 No, I’m joking. 03:25 So what do you find? You find your spherical nuclei and what do I mean by that bacon or sausage? Obviously, referring to your blood vessels. 03:33 You see those “rods”? Those are not rods, those are? Good. 03:38 Formation of new blood vessels and capillaries. 03:40 Clear? Angiogenesis. 03:42 You see this picture, no doubt you should reflexibly be able to identify this as being oligodendroglioma. 03:48 What if you find a palisading pattern that I showed you earlier as far as histology and it’s a primary CNS tumor? Then you should be thinking about glioblastoma multiforme. 03:58 I’m giving you specific histologic pictures that are extremely high yield for you. 04:03 I’m not going to give you every single histologic picture, that’s ridiculous. 04:07 So let’s stick with the ones that are high yield. 04:09 Could I give it to you? Well, absolutely. 04:12 But for the sake of time and efficiency, and for the sake of digestibility of the material, let’s somewhat keep this organized, please. 04:22 Neuroepithelial tumor that we’ll take a look at here is ependymoma. 04:26 Please think about your ependymal cells. 04:28 Now, what becomes important here is going to the age and location, that’s all that you need to know. 04:33 You’ll know exactly as to what you’re referring to. 04:36 Now, a couple of things here that I want to talk to you about with a child, the primary CNS tumor. 04:41 If I take you back to astrocytoma, what is the most common astrocytoma to be found in a child and where would it be located? You’re going to tell me -- I’m sorry. What did you say? Good. 04:53 Pilocytic type of astrocytoma. 04:56 Located where? Cerebellum causing then obstructive type of hydrocephalus, right? Good. 05:04 Here, we have another neuroepithelial tumor, but this time, this is an ependymoma. 05:08 Where is this located in a child? Fourth ventricle. 05:13 Do you have ependymal cells in the cerebellum? Well, if I had to compare the two, I would definitely put my bet on your fourth ventricle. 05:21 It may result here once again in hydrocephalus. 05:23 What kind please? Non-communicating, obstructive. 05:26 Take your time. 05:27 Understand it, don’t just memorize it. 05:31 Spinal cord is the most common location in which population? Adults. 05:36 Maybe by the cauda equina. 05:38 Once again, location and population is important. 05:42 And you’ll know about your ependymomas. 05:46 Let’s talk about a little bit more pathology about ependymoma. 05:49 Solid or papillary mass extending from the floor of the fourth ventricle. 05:53 Who? What do I mean who? Which population? What’s the population? Composed of cells with regular, round to oval nuclei with abundant granular chromatin. 06:03 A dense fibrillary background. 06:05 Tumor cells may form gland-like round or elongated structures. 06:10 We call these perivascular pseudorosettes. 06:14 Once again, perivascular pseudorosettes. 06:17 Why? The tumor cells form a gland-like structure around or elongated structure, perivascular. 06:24 And so therefore, it’s not a true rosette. 06:26 It’s a perivascular pseudorosette. 06:29 Because by rosette, you mean that you have the lumen, which would be extension of the cancer cells. 06:37 If you don’t know what a rosette is, well, a rosette is exactly as the name implies. 06:41 Think of a rose with petals, huh? So pretty. 06:45 When’s the last time you gave your significant other a rose? It might be time to do so. 06:50 And the inspiration was actually an ependymoma. 06:54 Anyhow, in medicine, we’re kind of sick, but whatever. 06:57 Well, some people say sick, some people say romantic, whatever. 07:01 Anyhow, so think of a rose with petals. 07:03 So the petals are the cancer cells. 07:05 So pretty. 07:06 And what’s the lumen? Well, if the lumen is an extension of the cancer cells, that is a rosette. 07:12 But if it’s a round perivascular, you can’t call that a rosette. 07:15 It is a pseudorosette. 07:17 It is a pseudorosette. 07:18 That is an important description here. 07:20 If it’s a child, most likely, where would you find an ependymoma? Good. 07:26 Floor of the fourth ventricle. 07:28 Where is it if it was an adult? Where would you find ependymoma? More or less in the spinal cord, maybe down by the cauda equina. 07:38 Clinical features: Hydrocephalus. 07:41 Is that confusing to you or is that crystal clear? If it’s a child, floor of the fourth ventricle, what are you going to cause? Obstructive, non-communicating type of hydrocephalus. 07:51 Poor prognosis, unfortunately. 07:53 Poor prognosis, unfortunately.
About the Lecture
The lecture Neuroepithelial Tumors: Oligodendroglioma by Carlo Raj, MD is from the course Tumors of the CNS. It contains the following chapters:
- Neuroepithelial Tumors: Oligodendroglioma
- Neuroepithelial Tumors: Ependymoma
Included Quiz Questions
The histopathological report of a 40-year-old man shows cells with spherical nuclei and finely granular chromatin and a surrounding area of clear cytoplasm. What is the most probable diagnosis?
- Oligodendroglioma
- Pilocytic astrocytoma
- Glioblastoma multiforme
- Meningioma
- Medulloblastoma
What is the most common location of an ependymal tumor in a child?
- Fourth ventricle
- Third ventricle
- Second ventricle
- Spinal cord
- Lateral ventricle
Which tumor has a dense fibrillary background and tumor cells forming gland-like elongated structures around the vascular area?
- Ependymoma
- Oligodendroglioma
- Meningioma
- Glioblastoma multiforme
- Pilocytic astrocytoma
Author of lecture Neuroepithelial Tumors: Oligodendroglioma

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
I love these lectures! Well structured and has a clean logical order
