Playlist
Show Playlist
Hide Playlist
Normal Pressure Hydrocephalus

-
Slides Other Dementias.pdf
-
Download Lecture Overview
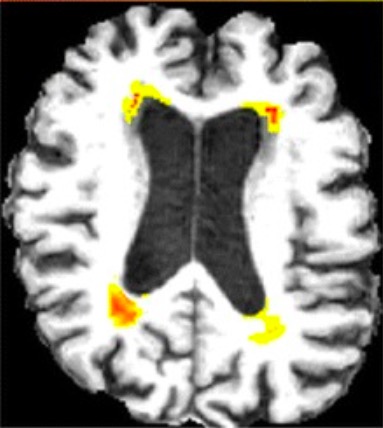
00:00 Now let's talk about normal pressure hydrocephalus. This is one of the important modifiable causes of dementia and movement dysfunction. In terms of epidemiology, this is the most common form of hydrocephalus, increase in fluid and ventricular size in adults. The incidence is 2 in 20 cases per million, so it's uncommon, but it is something that we see with the prevalence that increases with age usually over the age of 60 years. In terms of etiology what causes NPH, it's often idiopathic due to a combination of what's really poorly understood mechanisms, but there are some secondary causes. One of the most common is intraventricular subarachnoid hemorrhage which may alter CSF reabsorption permanently in those patients and contribute to this normal pressure hydrocephalus, enlarged ventricles with normal intracranial pressure long term, acute and chronic meningitis through some of the same mechanisms as well as a delayed effect of traumatic brain injury. So what's going on with NPH and how do patients present? Well, there is a classic clinical triad that you must know. And we think about the words wet, wacky, and wobbly. 01:16 Wet refers to incontinence. In early incontinence neurogenic bladder is common in patients with NPH and should tip us off to worry about this condition. Wobbly is gait ataxia. We see early gait ataxia. This is described as a magnetic ataxia, magnetic gait and can be severe and disabling and result in falls. And then wacky. 01:39 Memory disturbances and cognitive dysfunction are seen in these patients and that's one of the last symptoms to develop. We look to intervene in those early stages where incontinence or ataxia are present to reverse those symptoms. 01:53 By the time we're seeing cognitive dysfunction, our interventions may be less successful. And that typical clinical triad should prompt a work-up with imaging and/or CSF sampling to evaluate for NPH. In terms of imaging, it is critical for the diagnosis of NPH. We're looking for ventriculomegaly in the absence of atrophy. 02:15 We see enlarged ventricles if the brain is atrophic and that's called ex vacuo dilatation. As the brain shrinks, the ventricles accommodate that space. With NPH, we see ventriculomegaly in the absence of atrophy and there's a number of ways to define and measure this. One is by the Evans ratio and we're looking for a ratio of greater than 0.3. To calculate and evaluate the Evans index, we look at the widest interfrontal horn distance and compare that to the internal skull distance, and we'll look at that in the image in just a minute. Other imaging features that would be suggestive of NPH are the presence of temporal horns or enlargement of temporal horns. These are the temporal horns to the lateral ventricles which we usually don't see but prominent temporal horns indicate enlargement of the ventricular system. A callosum angle of 40 degrees of more, periventricular lucency but not ischemia and flow voids in the aqueduct to the 4th ventricle can also be suggestive. 03:19 Let's look at that Evans index on imaging and here on the far left in A we're looking at a calculation of the Evans index. We're comparing the size of the ventricles, that first line going from 1 to the other side of the ventricular system, the anterior horns of the lateral ventricles, and comparing that to the distance from one side of the skull to the other. And an Evans index of greater than 0.3 indicates enlargement of the ventricles for some reason which can be seen in NPH. 03:51 In addition to imaging, spinal fluid assessment can be important. This is a normal pressure hydrocephalus so we see that the opening pressure should be normal, less than 25-30 cm of water or 250-300 mm of water. When we evaluate these patients, we can perform a large volume LP. We can drain the spinal fluid to see if there's a clinical response and that's an important diagnostic test in evaluating for NPH. In addition to the spinal fluid opening pressure, we can also use a large volume LP to evaluate patients for NPH and their response to therapy. We look at the response to a large volume spinal tap where around 30-40 cc of spinal fluid is drained and we're looking for profound improvement in gait impairment. 04:41 Patients come in to the clinic, they undergo a walking assessment to look at the speed, number of steps and pace of their walking, they receive a large volume spinal tap draining off 30-40 cc of spinal fluid, and then that gait examination is repeated. 04:58 Patients who have significant improvement in their gait exam are more likely to respond to CSF shunting procedures which is one modality of treatment for these patients. And then in terms of treatment, we think about CSF shunting. 05:11 The problem in NPH is excess spinal fluid. We don't see that by increased pressure but we can see that as evidenced by ventriculomegaly and VP shunt is a consideration particularly in those patients who have response to a large volume spinal tap or continuous spinal fluid drainage.
About the Lecture
The lecture Normal Pressure Hydrocephalus by Roy Strowd, MD is from the course Other Dementias.
Included Quiz Questions
What is hydrocephalus?
- Increase in ventricular fluid and ventricular size
- Increased intracranial pressure and increased ventricular size
- Enlarged head circumference with imaging correlation
- Clinical syndrome of "wet, wacky, and wobbly"
Which of the following is a major secondary cause of normal pressure hydrocephalus? (Select all that apply.)
- Subarachnoid hemorrhage
- Acute and/or chronic meningitis
- Chronic ischemia
- Acute stroke
- Alzheimer dementia
What is the classical clinical triad seen in normal pressure hydrocephalus?
- Incontinence, magnetic gait ataxia, behavioral disturbances ("wet, wobbly, wacky")
- Scanning speech, intention tremor, nystagmus
- Bradycardia, bradypnea, hypertension
- Ptosis, miosis, anhidrosis
What are the classic neuroimaging findings of normal pressure hydrocephalus?
- Ventriculomegaly in the absence of atrophy
- Periventricular enhancement (Dawson fingers)
- Cortical atrophy with ventricular enlargement
- Atrophy of the corpus callosum and scattered white matter enhancement
Author of lecture Normal Pressure Hydrocephalus

Roy Strowd, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
