Playlist
Show Playlist
Hide Playlist
Nocardia Species

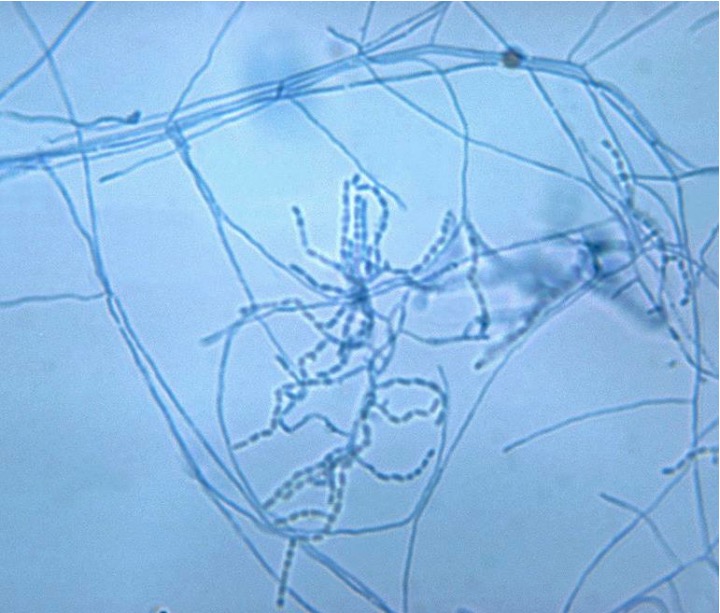
00:01 Nocardia Species, a bacteria. 00:03 Nocardia are gram-positive rods which fairly unusually are branching and look a bit like mold or they have mold-like filaments. 00:12 In fact, the nocardia frequently can't figure out exaclty what they wish to be called as. 00:17 But they are indeed bacteria with many characteristics of other types of organisms. 00:22 They are obligate aerobes and they live extensively in the soil. 00:27 In fact, anywhere you look any part of the world one can find nocardia species. 00:31 Importantly, they are slow growing which also means the diseases associated with nocardia, frequently are slow in onset. 00:40 They have a wax-like outer layer which also produces some mycolic acid. 00:46 Both of these are features typically more often found in fungus. 00:50 Because they produce some mycolic acid, it takes up acid-fast stain. 00:55 So nocardia are traditionally known as partially acid-fast stain organisms. 01:01 They also do produce urease and catalase. 01:04 How do nocardia produce disease? First and foremost is through inhalation. 01:12 And especially nocardia asteroides. 01:15 As the nocardia is inhaled perhaps through the soil or blown dust, etc., they can colonize the oropharynx. 01:24 At some point it maybe aspirated into the lower airways which traditionally and typically are sterile. 01:32 In patients who have some problem with immunity whether their immunosupressed through medication or immunocompromised through a disease they may develop active disease related to this aspiration. 01:45 That disease typically causes and is associated with necrosis and an abscess formation of the lungs. 01:52 In other exposures, more typically in immunocompetent people an environmental exposure occurs typically a soil or dirt contamination of a wound which then creates a slow growing wound infection. 02:07 Importantly, this is also a slow process, so unlike a typical cellulitis with other bacteria, nocardia skin infections are very slow in nset. 02:18 And they'e associated with granulomas on pathology. 02:22 Here if we look a bit more closely at the respiratory disease, the bronchopulmunary disease caused by nocardia, the classic subspecies of nocardia is asteroides. 02:34 In patients who aspirate nocardia asteroides into their oropharynx and down into their lungs, they may develop a caseous necrosis. 02:44 Caseus, cheese-like which is very much a reference to how these lesions look like on gross microscopy. 02:51 In fact, if you look at patients with pulmonary or bronchopulmonary nocardia disease it mimics extensively tuberculosis caused by mycobacterium tuberculosis. 03:03 However such patients have negative testing for tuberculosis such as with the PPD skin test. 03:09 Patients with bronchopulmonary nocardia will typically start with a mild non productive cough which is associated with low grade fevers, dyspnea or shortness of breathe and then eventually develop further signs of pneumonia with a cavitary or whole producing lesion inside the lungs. 03:29 If they are immunocompromised or altered immunity such as they are very young or very old the disease may enter the lymph or the blood system and travel to the central nervous system. 03:41 Patients with proven nocardia lung disease must also be evaluated for brain abscesses. 03:48 For patience with cutaneous infections, again transmission via a normal skin wound, an abrasion or laceration from soil or dirt and here these are lesions typically caused by nocardia brasiliensis. 04:03 Again super infection of a wound causes a chronic slow progressing infection which is or appears to be almost like wart-like. 04:15 This patients have associated swelling in the deep tissues, the subcutaneous layers and ultimately if for a long period of time may develop a chronic draining purulent infection, with sinus tracts such as you see in the picture on the right side of the slide. 04:33 In fact, compared to other infections which also produce chronic slowly progressing infections, nocardia is almost indistiguishible from such infections and these are microbacterial infections, cutaneous disease in fact and sporothrix or sporotrichosis is the name of that disease. 04:54 Treatment. 04:55 Typically treatments can be long term treatment with sulfonomide antibiotic and by long term we're talking weeks to sometime months. 05:04 If the patient has a sulfuric reaction, an allergic reaction to the sulfur component, other antibiotics are possible such as Amikacin, tetracycline, including minocycline, and occasionally a third generation cephalosporin. 05:18 But all of these are less ideal than primary treatment with the sulphide drugs. 05:23 In the case of cutaneous disease surgical intervention is quite necessary. 05:28 All these together are the way to go for long term treatment of a long term infection but the key part is to recognize nocardia infection when it causes respiratory disease and distiguish it closely and carefully from tuberculosis as it represents a whole different approach to disease management.
About the Lecture
The lecture Nocardia Species by Sean Elliott, MD is from the course Bacteria.
Included Quiz Questions
Which of the following best describes the typical cutaneous lesions produced by infection of wounds by Nocardia species?
- Granulomatous lesions
- Nodular lesions
- Vesicular lesions
- Petechial lesions
- Plaques
Bronchopulmonary disease occurring in an immunocompromised individual due to infection with Nocardia asteroides characteristically produces which of the following types of necrosis?
- Caseous necrosis
- Liquefactive necrosis
- Coagulative necrosis
- Fat necrosis
- Fibroid necrosis
Which of the following species belonging to the Nocardia genus is most commonly implicated in the manifestation of mycetoma in wound infections?
- Nocardia brasiliensis
- Nocardia asteroides
- Nocardia africana
- Nocardia brevicatena
- Nocardia blackwellii
Author of lecture Nocardia Species

Sean Elliott, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
