Playlist
Show Playlist
Hide Playlist
Neonatal Abstinence Syndrome (NAS)

-
Slides NeonatalAbstinenceSyndrome Pediatrics.pdf
-
Download Lecture Overview
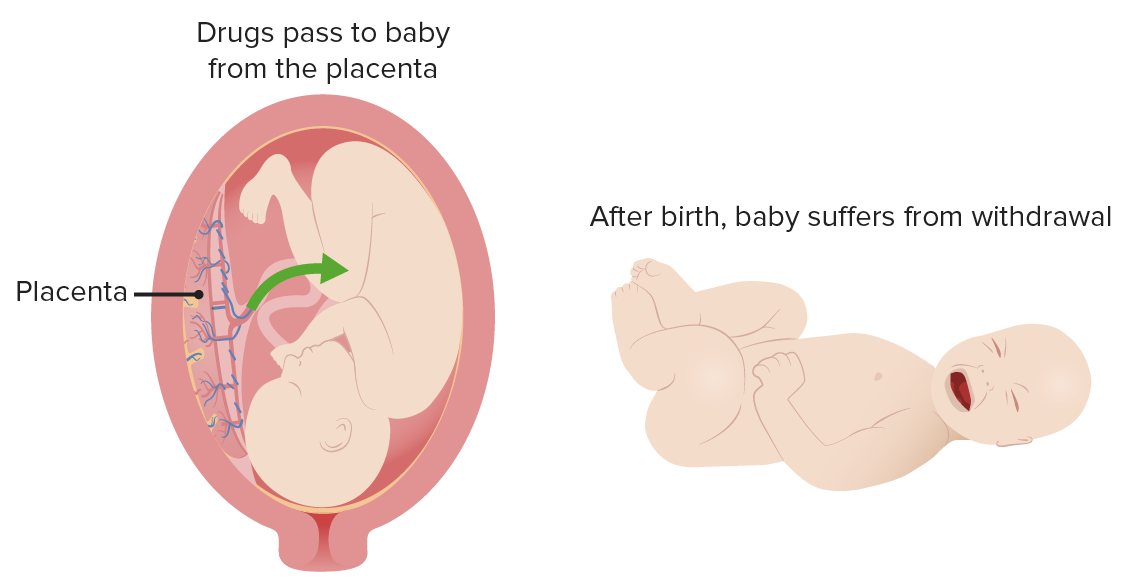
00:01 In this lecture, we’re going to discuss the neonatal abstinence syndrome. 00:07 So basically, in utero drug exposure in U.S. pregnant women is very high. 00:14 4% percent of pregnant women use illicit drugs, 11% percent use alcohol, 4% percent admit to binge drinking, and 16% percent smokes cigarettes. 00:25 We have a problem in the United States with pregnant women ingesting substances that are inherently bad for infants. 00:32 Especially on the rise is illicit use of opiates. 00:36 And that epidemic in the United States is causing a wide outbreak of infants with neonatal abstinence syndrome. 00:45 Let’s look through the illicit drugs in pregnancy and what they do. 00:49 There is growing evidence that smoking marijuana during pregnancy may be associated with lower birth weight Cocaine and methamphetamine can cause prematurity. 01:00 They can make infants small for gestational age and they can give infants IVH or bleeds inside their head. 01:10 Heroine can cause stillbirth. 01:13 It can make infants small for gestational age. 01:16 It can result in SIDS or sudden infant death syndrome and it can create neonatal abstinence syndrome, which we’re going to spend the bulk of this conversation on. 01:27 So let’s talk about neonatal abstinence syndrome. 01:30 This is a nonspecific CNS and autonomic nervous dysfunction. 01:36 It’s a result of in utero exposure to opiates. 01:40 And then abrupt cessation at delivery. 01:43 It’s like making a newborn go through withdrawal. 01:47 The symptoms typically begin one to two days after birth. 01:52 So here is the list of some of the symptoms we have to contend with in these infants. 01:57 They have vomiting, the have diarrhea, they have uncoordinated and inconstant suck. 02:03 Or they suck very frequently, but it’s uncoordinated so they aren’t getting the breast mild they need. 02:09 Thus, they may have poor wait gain. 02:12 They get irritability, jitteriness, a shrill cry. 02:17 They may have hypertonia or have myoclonic jerks or they may frankly seize. 02:22 Additionally, they can develop fever, which is perhaps the most annoying part of it because the fever can be misinterpreted as an infection and then create an entire rule out sepsis. 02:34 They may have sweating, they may have tachycardia, they may have tachypnea and one classic thing is nasal stuffiness. 02:43 So if we see an infant where we suspect withdrawal, we will do a score. 02:48 There are several scores out there and the score that’s used in your center is probably the best one for you to be using. 02:55 The Finnegan score, the Lipsitz score, the neonatal withdrawal index. 02:59 I suspect the Finnegan is probably the most popular. 03:02 So if you look at Finnegan, there are literally eighteen different symptoms that usually a nurse will score. 03:10 For example, they’ll score how much nasal stuffiness they have and that will give them a point or two. 03:16 Or they might say something about how bad is the diarrhea or how bad is the vomiting and it’s basically 18 points. 03:22 They take the points and then they add them all up and that gives them a score. 03:27 You will not on an exam be asked to recapitulate one of these scoring systems or to calculate a score in an infant, but you will definitely need to know that these scores are what we are using to track improvement or to make a diagnosis in the first place. 03:43 We’re going to use these scores to have us decide exactly how much we should dose the infant in terms of the morphine we’re going to be giving this infant back and then we’ll use them also to track our gradual withdrawal of the morphine to see when they’re safe to be weaned further. 04:02 So we also do non-pharmacologic therapy. 04:07 There are a lot of things we can do to these infants who are very fussy to make them feel better and feeling better is important. 04:14 This infant didn’t ask to go through withdrawal. 04:17 So swaddling is critical. 04:19 These kids loved to swaddled and we should do it. 04:22 Rock them, not in a swing-like this. 04:25 I mean one of those little baby swings that goes back and forth. 04:29 We should avoid excessive sensory or environmental stimulation. 04:34 So for example, we shouldn’t have them too irritated or bothered. 04:39 Don’t let all the friends and the family come in and examine the child. 04:43 We should minimize their sensory environment and just keep them in a warm, comfortable place. 04:49 Maintaining temperature stability is important because these infants can get cold very quickly. 04:56 Also, remember, feeds are comforting. 04:59 So we want to breastfeed if possible, keeping in mind that excessive sucking is often non-nutritive. 05:06 It doesn’t mean the child’s hungry, it’s just part of their symptoms of withdrawal. 05:11 So what do we do with the medications? Well, the key is morphine. 05:16 And what we’ll do is we’ll put them on morphine to the point where they’re at an appropriate Finnegan’s score. 05:21 Then we will engage in a gradual wean by about 10% per day. 05:27 Slowly bringing them down to a point where now they can come off and everything will be fine. 05:33 If the infant has a higher score, we will give a breakthrough dose and if that happens a lot, we may bump up the daily dose so we can keep them on a controlled wean. 05:44 Many people use phenobarbital. 05:46 This is an additional therapy for polysubstance exposure or in combination with morphine, for an infant that’s having a hard time coming off the morphine. 05:58 Another key thing is treating the mother for addiction. 06:02 Remember that opiates in mom get into the breastmilk and they complicate the picture. 06:07 Also, an addicted mother may have problems in terms of raising that child and she may need more help to help her get off this very addictive substance. 06:17 So that’s a critical part of caring for these infants. 06:20 So that’s my review of neonatal abstinence syndrome in children. 06:24 Thanks for your time.
About the Lecture
The lecture Neonatal Abstinence Syndrome (NAS) by Brian Alverson, MD is from the course Neonatology (Newborn Medicine).
Included Quiz Questions
Which of the following is NOT a symptom of opiate withdrawal in infants exposed to drugs in utero (Neonatal Abstinence Syndrome) ?
- Excessive weight gain.
- Sleep & wake disturbance.
- Feeding difficulties.
- GIT disturbance (vomiting & loose stool).
- Tremors.
Author of lecture Neonatal Abstinence Syndrome (NAS)

Brian Alverson, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
2 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
great lecture great teacher great lecture great teacher great lecture great teacher
Excellent lecture as usual. Very easy to understand and remember the symptoms and management.
