Playlist
Show Playlist
Hide Playlist
Neisseria Meningitidis

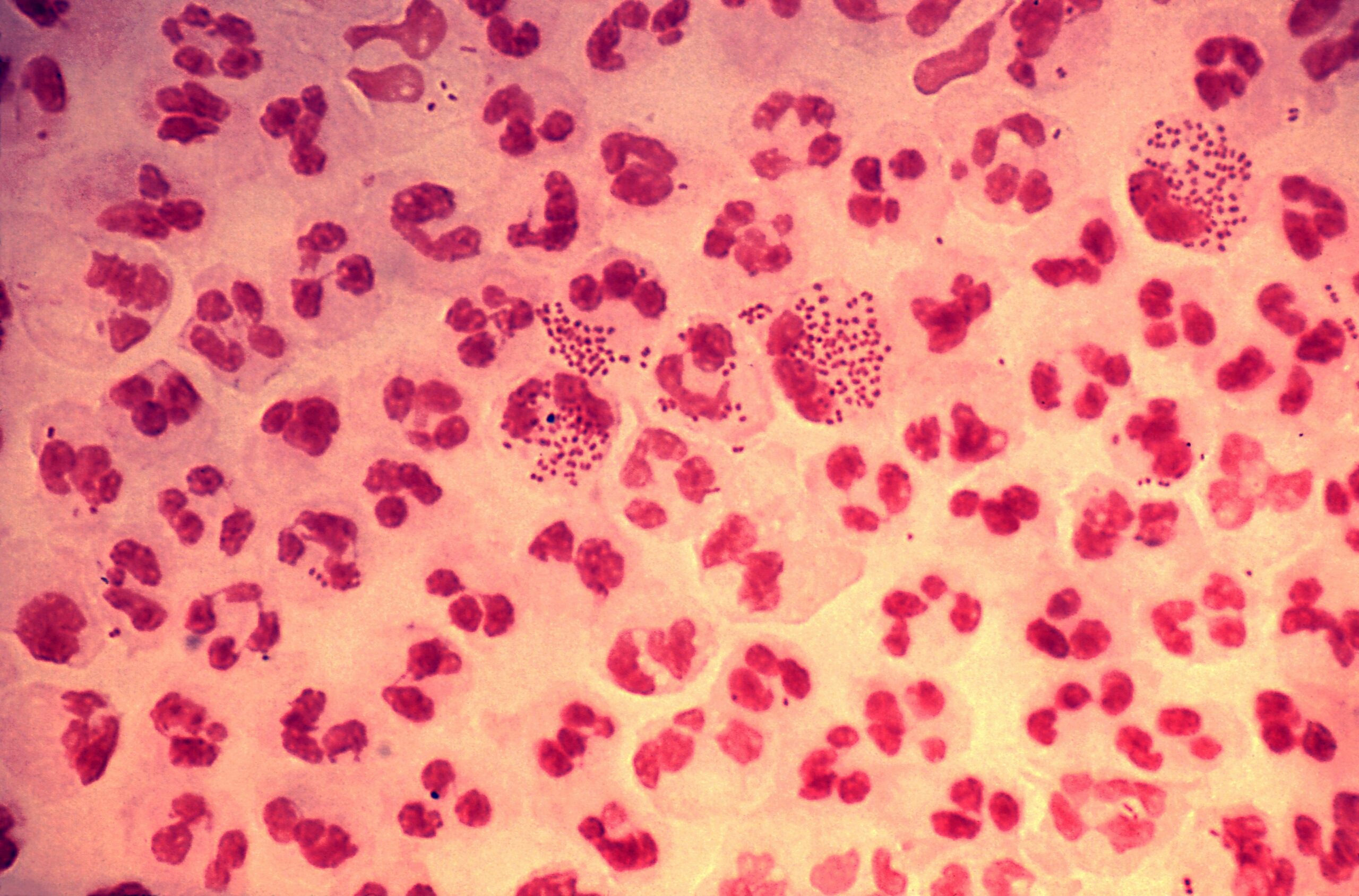
00:01 Neisseria species, a bacteria. 00:03 Neisseria, are gram-negative diplococci which appear on gram-stain like kidney beans facing each other such as you see on this picture here. 00:14 This picture shows neisseria meningitidis. 00:17 This one shows neisseria gonorrhoeae, another important form of neisseria. 00:23 Both, however, appear to be facing kidney beans. 00:27 Neisseria meningitidis which we'll spend our time talking about in this section, are typically known by their serogroup positivity. 00:38 This slide demonstrates the typical outer structure of Neisseria Meningitidis, including pilots structures, capsular polysaccharides, outer membrane proteins and lipid oligosaccharides in the outer membrane which contains the lipid A which functions as a lipid based endotoxin. 00:56 Neisseria Meningitidis usually is classified into various groups, however, based on its polysaccharide capsule. 01:03 The most common types being A, B, C, X, Y, Z, W135 and L. 01:11 The most important testable facts. 01:13 So the thing to remember for these variants is that the polysaccharide capsule of Serogroup B has a very poor immune response a that has made it a difficult target for vaccine discovery, but also that vaccine for meningococcal type B targets membrane proteins as opposed to the capsule antigens. 01:33 As noted before, Neisseria meningitidis are gram-negative diplococci and you can see a beautiful picture on this slide, looking almost like owl's eyes, not the classic pathologic definition, but looking like two-kidney shapes facing each other. 01:49 On culture, the organism itself is non-motile, it does not swim about. 01:54 Diplococci or paired cells are typically how the organism is shown. 02:00 It would be rare to see individual gram-negative cocci by themselves. 02:04 The organism is pretty much everything-positive: maltose, oxidase, and catalase. 02:10 Lipooligosaccharides create endotoxin activity mostly which create this endotoxin activity mostly by precipitating a proinflammatory cytokine reaction. 02:20 The organism itself ferments both maltose and glucose as noted above and in the growth, it is especially able to grow on a chocolate-based agar, typically the Thayer-Martin agar. 02:32 Neiserria meningitidis is incredibly contagious. 02:37 Unfortunately, it can be presented and acquired through respiratory droplets as well as occasionally via large droplets which is come to rest on a horizontal surface. 02:48 Patients who are most at risk of developing disease from Neisseria meningitidis are those with terminal complement deficiencies, C5 to C9. 02:58 However, anybody can get disease with Neisseria meningitidis especially including those who are the very young, children less than five, and those who are a little bit older. 03:09 There's a specific at-risk patient population that are those young adults attending college in the first one or two years. 03:16 Exactly why is not known and that specific age association has not been definitely proven by evidence-based medicine. 03:24 However, factors that are important may be close proximity, i.e., going out for drinks after school, smoking cigarettes which compromises respiratory cilia as in, defense mechanism, and fatigue, being up at all hours studying, I'm sure, no partying involved in young college students. 03:45 Put all those factors together, may precipitate that particular risk. 03:50 On this slide, we see a graph of the so-called meningitis belt, including areas at high epidemic risk in sub-Saharan Africa. 03:59 The dark shaded band across the middle of the sub-Saharan part of Africa demonstrates areas at high epidemic risk. 04:06 The lighter shade of gray for those countries shows areas with increased risk for meningitis due to meningococcal disease. 04:16 How does the disease occur? How does neisseria meningitidis do what it does? The first step is to enter the respiratory tract then it invades the mucosal membranes and ultimately enters the bloodstream. 04:30 So, a several step process which requires there to be organism which enters into the bloodstream for it to actually cause disease. 04:37 Once entering the bloodstream, an organism proliferation occurs then Neisseria meningitidis starts to release endotoxin, and it is that endotoxin along with the proinflammatory cytokine reaction to its polysaccharide capsule, which creates the sepsis: fever, increased vascular permeability, followed by leakage of fluids, shock, and then localized bleeding causing petechiae. 05:05 The antiphagocytic capsule, as mentioned, is also important not only in inducing proinflammatory cytokines, but also in avoiding detection by and ingestion by phagocytes. 05:18 So, several mechanisms of virulence occur in the setting of neisseria meningitidis. 05:24 Diseases that it causes: perhaps the most fearsome is meningitis, an easy one to remember because it's in the name. 05:31 Typical meningitis is, as you would anticipate, an acute onset of fever, followed by a severe headache and a stiff neck. 05:40 Importantly, some patients, especially children, are unable to report or even demonstrate on physical exam evidence of a stiff neck so instead, one sees evidence of extreme irritability. 05:52 Along with meningitis, patients may have what's called acute meningococcemia. 05:58 This simply means by its name, presence of the organism, Neisseria meningitidis organism, within the bloodstream, creating its endotoxin and its capsular virulence. 06:11 Patients with meningococcemia will have septicemia or septic shock. 06:16 They may or they may not have active meningitis. 06:20 Patients with the -- the disease process will present with acute onset fever but rapidly progress into shock, generalized hemorrhage such as you see on the picture of the baby to the right, along with diffused purpura lesions, and discrete petechiae, and they will also have multi-organ dysfunction. 06:40 The only way to survive meningococcemia is to have it be promptly recognized and treated empirically. 06:47 The mortality or the death rate is at least 25% and untreated, it approaches 100%. 06:55 There is a less severe form of disease caused by neisseria meningitidis which is called chronic meningococcemia. 07:03 Unfortunately, that name, meningococcemia, strikes fear in the hearts of clinicians because it is so overtly associated with bad outcomes. 07:13 But chronic meningococcemia is not severe and is not typically fatal. 07:18 Typically, these patients have circulating bacteremia, circulating Neisseria meningitidis for several weeks at a time. 07:26 And then, they may develop low-grade fevers sometimes with arthritis or even just arthralglas, painful joints. 07:34 And then as the fevers subside for a week or so, they may develop petechial skin lesions such as you see on the legs of one of my patients on the picture to the right. This is a mild illness. 07:46 It is not known to progress to severe disease, except in rare instances when the patient develops compromised immunity. 07:54 And then, they may enter full fledged acute meningococcemia with all the attendant morbidity and mortality that we just described. 08:03 So, a mild febrile disease. 08:05 Also, in addition to chronic meningococcemia, patients can develop a transient, short-lived pharyngitis illness, which may also be associated with other evidence of serositis. 08:18 So, the serosa, the pleura lining various organs such as the lungs, the joints, the urethra, can become inflamed and these are patients who are acutely ill as you might be with the flu for several days and then spontaneously improve. 08:36 A horrible complication of meningococcemia is known as the Waterhouse-Friderichsen Syndrome. 08:42 And in this case, there is an addition to the already-severe disease with acute meningococcemia, there is an overwhelming immunologic reaction to the polysaccharide capsule, which is associated with disseminated intervascular coagulation disease or DIC with bilateral hemorrhagic adrenal infarcs, septic shock, acute hypotension, all of the above, along with cardiac dysfunction, tachyarrhythmia, etc., and so forth. 09:12 And these patients, in addition to having purpuric disease, will also have petechial disease. 09:19 This is a process which, even if recognized, is very difficult to reverse and extremely fatal to those who suffer from it. 09:28 So, prevention. Well, the best prevention of course is to avoid exposure in the first place. 09:35 Although, that may not be necessary, so it may not be possible. 09:39 However, creating an immunologic prevention is the next best step. 09:45 Exclusive breastfeeding, transfer of maternal immunity for the first six months of life is always a good idea. 09:53 Although, the mother may not herself have been exposed to Neisseria meningitidis, she may have been low-level exposed from other people and thus have some partial immunity to transfer to her baby. 10:08 For those who don't have the benefit of that exposure, there is now an immunization or a vaccine product which is conjugated to a protein to induce an exaggerated and effective seroprotective response. 10:22 Several products are on the market. 10:24 All of them are licensed and in use for children ages two years of age and older. 10:30 However, they are effective down to two months of life However, they are effective down to two months of life The quadrivalent meningococcal conjugate vaccines, which can be meningococcal ACWY are indicated for eligible groups. 10:43 These include all pediatric patients ages 11 to 18 years of life, as well as children ages two months to ten years of life or through ten years of life who have an increased risk for meningococcal disease. 10:55 The high risk categories include those with persistent terminal complement deficiencies taking a complement inhibitor such as Soliris, those with anatomic or functional asplenieas such as sickle cell disease, traumatic splenic etc. 11:12 Those with active HIV infection regardless of treatment, and those who reside in a hyper endemic or epidemic region, especially if they'll have prolonged contact with the local population. 11:24 For those patients who are exposed to Neisseria meningitidis, because it is so highly contagious and because it is so robustly associated with various severe disease, those are patients who do deserve antibiotic prophylaxis. 11:38 Most commonly, the drug rifampin is used. 11:40 Although, quinolones such as ciprofloxacin or sulfonamides are also used to prevent that disease process. 11:49 And so Neisseria meningitidis is associated with most often very severe disease, highly contagious, occuring at those who are most at risk, it can also cause a more chronic form, but regardless of the situation, When one sees gram-negative diplococci or kidney bean faced or gram-negative rods facing each other, one should be very worried and start treatment right away for the possibility of meningococcemia. 12:17 And so, treatment. Historically, penicillin was the treatment of choice for all of the Neisseria species: meningitidis, gonorrhoeae, etc. 12:27 Unfortunately worldwide, many reports now exist of penicillin resistance. 12:32 And so the alternatives: broad-spectrum cephalosporins, most especially the drug ceftriaxone, as well as, in parts of the world that have access to this, chloramphenicol and sulfonamides are the treatment of choice. 12:45 While empiric treatment is not something in terms of antibiotic overuse that we wish to indulge in too frequently, in the case of meningococcemia, where the outcomes are so uniformly horrible and the onset and progression disease is so rapid, empiric treatment is indicated in this specific circumstance.
About the Lecture
The lecture Neisseria Meningitidis by Sean Elliott, MD is from the course Bacteria.
Included Quiz Questions
On gram staining of a specimen obtained from an individual infected by Neisseria species, which of the following would you expect to find?
- Gram-negative diplococci
- Gram-positive diplococci
- Gram-negative bacilli
- Gram-positive bacilli
- Gram-positive monococci
Which of the following refers to the shape of bacteria observed on microscopic evaluation of a specimen obtained from an individual infected by Neisseria meningitidis?
- Paired kidney-shaped bacteria facing each other
- Spindle-shaped bacteria
- Club-shaped bacteria
- Bullet-like bacteria
- Brick-shaped bacteria
Which of the following culture media allows the best growth of Neisseria meningitidis?
- Thayer-Martin agar
- Baird-Parker agar
- MacConkey agar
- Hektoen enteric agar
- Mannitol salt agar
The species of Neisseria genus which is most likely to cause Waterhouse-Friderichsen syndrome is...?
- ...Neisseria meningitidis.
- ...Neisseria gonorrhoeae.
- ...Neisseria lactamica.
- ...Neisseria flavescens.
- ...Neisseria wadsworthii.
Which type of vaccine is most commonly used for the prevention of Neisseria meningitidis infection?
- Conjugate
- Toxoid
- Live attenuated
- Killed/inactivated
- Recombinant
Which of the following tuberculosis drugs is commonly used for prophylaxis after exposure to Neisseria meningitidis?
- Rifampin
- Ethambutol
- Isoniazid
- Pyrazinamide
- Streptomycin
Author of lecture Neisseria Meningitidis

Sean Elliott, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
sooooo sooo good!!! i understoof everything and is amazing that he included everything important about this bacteria! great teacher!
