Playlist
Show Playlist
Hide Playlist
Natural History and Progression of Alzheimer Dementia

-
Slides Alzheimer Dementia.pdf
-
Download Lecture Overview
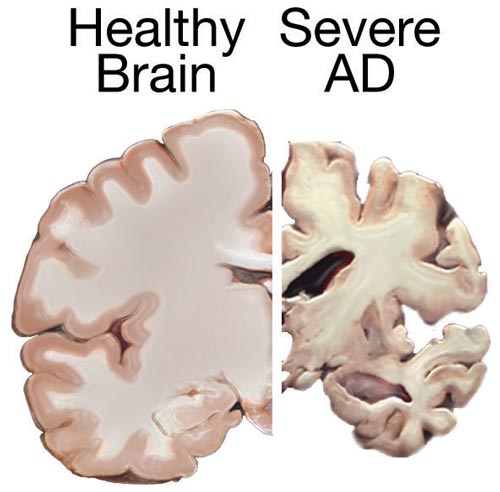
00:00 If we look at what's happening over time, we see there's a period where patients are asymptomatic. Subsequently, patients will develop short-term memory loss, followed by loss of other motor language skills ultimately progressing to patients becoming bedridden and eventually death. And these brain changes that are occurring are very early in the disease. In fact, really developing during this asymptomatic. 00:27 Early in the asymptomatic period, we see the development of neuritic plaques, that's that beta-amyloid build-up. This is followed by microglial activation, again very early in the course of the disease, tau pathology in the form of neurofibrillary tangles develops, and subsequently there is synaptic dysfunction, reduction in synaptic density, and decline in neurologic function. And importantly, all of that pathology that's developing on the brain is doing so during that asymptomatic and pre-symptomatic period. So by the time patients present with symptoms, the pathology is there and it's a very difficult disease to turn back time. If we look at this graphically, here we can see the stages of build-up of this pathology over time and the duration of these phases. In the middle, the dash line is the onset of cognitive impairment clinical symptoms. And we see that that really correlates with synaptic and neuro function and density in the decline in the number of synapses in the function within the synapses. This is a late finding in patients. 01:31 Already, we have significant accumulation of the brain of beta-amyloid and tau as well as microglial activation. And so when we're thinking about therapeutic interventions to disease modify, modify the development of Alzheimer's disease, we really are looking to treat patients during this pre and asymptomatic period of time. When we think about Alzheimer's dementia, beta-amyloid and tau are the important proteins involved and they have a predilection for certain areas of the brain. Primary age-related tauopathies do occur. This is age related cognitive decline and build-up of tau and primarily occurs in the parahippocampal gyrus as well as some areas of the brainstem. In Alzheimer's disease, we see early development in deposition of beta-amyloid and to some degree tau in the medial prefrontal cortex as well as the medial parietal cortex contributing to early visual spatial dysfunction in these patients. As Alzheimer's disease progresses, we see trafficking of tau throughout the brain initially in the hippocampus, parahippocampal regions contributing to memory dysfunction and then ultimately up into the parietal lobe contributing to prominent visual spatial dysfunction. Patients get lost when driving, get confused when they're navigating, have difficulty with navigation and transportation as a result of those visual spatial symptoms that occur from where tau and amyloid beta are depositing in the brain. As we put this altogether, we can look at the clinical symptoms, our ability to diagnose biomarkers of the disease and the pathologic changes that are occurring. When patients present with clinical symptoms particularly with functional impairment, we can make a diagnosis of dementia which is actually occurring very late in the course of this disease. 03:18 Cognitive dysfunction may develop slightly earlier and contribute to a diagnosis of MCI but there is a prominent preclinical period of time where important things are happening. We can look for those with biomarkers. Standard anatomic imaging does a poor job of evaluating early preclinical symptoms and MRI really only shows advanced atrophy in that late dementia phase. We can use FTG PET or CSF tau levels or amyloid beta imaging to start to image earlier some of the pathology that begins in the early symptomatic and pre-symptomatic windows. Ultimately, the pathologic changes are beginning well before symptoms both in terms of accumulation of tau and amyloid beta. And you can see down at the bottom the onset in the number of years of some of these changes prior to the development of patient's symptoms.
About the Lecture
The lecture Natural History and Progression of Alzheimer Dementia by Roy Strowd, MD is from the course Alzheimer Dementia.
Included Quiz Questions
Concerning the pathophysiology of Alzheimer dementia, what is hypothesized to be the first and most important step in its development?
- Formation of beta-amyloid plaques
- Formation of neurofibrillary tangles
- Microglial activation
- Head trauma
By the time clinical symptoms have developed in patients with Alzheimer disease, which of the following pathophysiologic steps might you expect to have already occurred?
- All of the answer options are valid.
- Beta-amyloid plaque accumulation
- Microglia activation
- Neurofibrillary tangle formation
What anatomic portion of the brain dictates our visual-spatial understanding?
- Parietal lobe
- Frontal lobe
- Temporal lobe
- Hippocampus
- Occipital lobe
What anatomic portion of the brain dictates our ability to form and retain memories?
- Hippocampus
- Amygdala
- Frontal lobe
- Broca's area
- Mammillary bodies
Author of lecture Natural History and Progression of Alzheimer Dementia

Roy Strowd, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
