Playlist
Show Playlist
Hide Playlist
Myasthenia Gravis: Introduction and Clinical Features

-
Slides Strowd Myasthenia Gravis.pdf
-
Download Lecture Overview
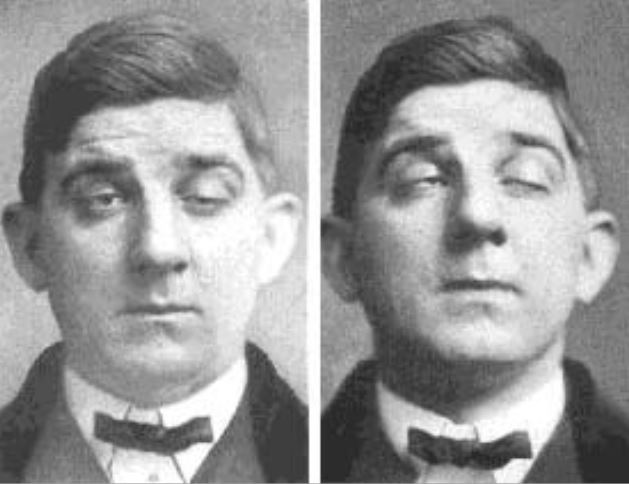
00:01 So what is Myasthenia Gravis? Let's talk a little bit more about this condition. 00:05 This is an autoimmune disorder, so it's immune mediated, with systemic autoantibodies to the postsynaptic acetylcholine receptor complex. 00:14 In general, patients present with weakness. 00:17 That's the chief complaint. 00:19 And with additional questioning and an examination, we see prominent bulbar findings. 00:23 Ptosis, diplopia, dysarthria, dysphasia, and other evidence of bulbar muscle dysfunction. 00:29 Often with fatigability that may be present on history, or evaluated on our examination. 00:35 And here you can see a representative picture of a patient who has right sided ptosis, which should point us in the direction of a junctional disorder and away from muscle. 00:45 What are some of the key features of patient's clinical presentation? Well, the weakness can be in any distribution. 00:51 It can be proximal, it can be distal, it can be symmetric, it can be asymmetric. 00:56 But importantly, we see prominent bulbar findings. 00:59 What is the fatigability look like? Well, symptoms may be worse at night or after exercise. 01:05 Patients may describe that when they walk into the grocery store, they don't have a lot of weakness, or diplopia, or dysarthria but that's more prominent the end of their shopping. 01:14 Reading may be easier at the beginning of a book and much more difficult at the end of a chapter where diplopia may be pronounced. 01:22 Ptosis may be evident on this exam with sustained upgaze. 01:26 And we perform this on our examination. 01:28 Evaluating the ability to sustain upgaze and looking for ptosis or sustained muscle contraction and looking for fatigability on our generalized motor exam. 01:38 And weakness may be more prominent with prolonged muscle contraction. 01:43 Here we see another patient with prominent ptosis bilaterally, right worse than left. 01:49 No meiosis. 01:50 The pupils are both the same size and are normal. 01:53 But we see prominent ptosis. 01:54 A problem with muscle function in the bulbar area. 01:58 And importantly, their sparing of autonomics. 02:01 We don't see parasympathetic dysfunction, which we can see with other junctional disorders and problems in other areas. 02:08 As we see here, some of the presenting symptoms that we should look out for are diplopia and ptosis. 02:13 Present in 50 to 64, 65 or so percent of patients. 02:17 Generalized weakness is common, but not present in all patients. 02:21 We see the prevalence of both leg weakness, fatigue and respiratory failure, though uncommon, is important to recognize because this can contribute to substantial morbidity and even mortality in these patients. 02:32 When we think about myasthenia we can categorize it in a number of different ways. 02:37 There is generalized myasthenia and ocular myasthenia. 02:40 Some patients have prominent weakness all over the body. 02:43 With weakness of the legs, and the arms, as well as the bulbar findings. 02:48 In generalized myasthenia includes generalized weakness with bulbar symptoms. 02:53 In contrast, ocular myasthenia tends to affect the eyes more prominently. 02:57 Patients who may have very limited systemic weakness or no systemic weakness at all, but prominent ptosis and potentially other bulbar symptoms. 03:08 We can also categorize myasthenia into the result of serologic test. 03:12 There's acetylcholine receptor positive, and other types of seronegative or other antibody positive myasthenia. 03:19 Acetylcholine receptor antibody positive myasthenia presents with prominent proximal weakness, facial dysfunction, bulbar symptoms and respiratory weakness can be seen in this condition and should be evaluated in these patients. 03:33 Muscle-specific kinase is a different part of the acetylcholine receptor that can be damaged or dysfunctional. 03:41 And MuSK-specific myasthenia tends to present in younger women, predominantly with facial bulbar or respiratory weakness with an absence of generalized weakness in some of these patients. 03:53 And again, there's relatively mild limb weakness with MuSK-positive myasthenia.
About the Lecture
The lecture Myasthenia Gravis: Introduction and Clinical Features by Roy Strowd, MD is from the course Disorders of the Neuromuscular Junctions.
Included Quiz Questions
Which of the following clusters of symptoms most closely aligns with the diagnosis of myasthenia gravis?
- Ptosis, dyspnea from weakness of respiratory muscles, and a worsening of symptoms with muscle use
- Proximal muscle weakness, dry mouth, impotence
- Ptosis, diplopia, muscle weakness that improves with use
- Chronic widespread pain associated with “tender points”
- Pain and stiffness in proximal muscles, often with fever, malaise, and weight loss
Which of the following is the most common presenting symptom of myasthenia gravis?
- Diplopia/ptosis
- Autonomic symptoms
- Weakness
- Fatigue
- Respiratory failure
Author of lecture Myasthenia Gravis: Introduction and Clinical Features

Roy Strowd, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
