Playlist
Show Playlist
Hide Playlist
Myasthenia Gravis in Children

-
Slides Muscle Disorders in Children.pdf
-
Download Lecture Overview
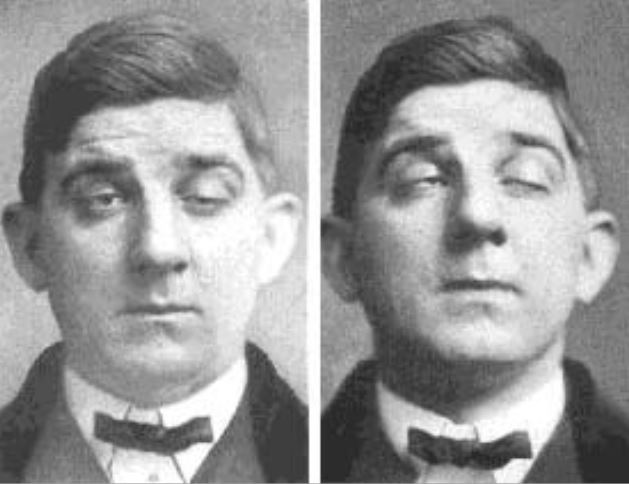
00:01 Let's switch to Myasthenia Gravis. 00:04 Many students think of Gravis as an adult disease. 00:07 But there are absolutely, rarely pediatric variants both in the newborn period and later on in childhood. 00:16 Myasthenia Gravis of the newborn it presents as a chronic muscle weakness with fatigability. 00:23 This is an autoimmune attack of antibodies against the Acetylcholine receptors in the post synaptic muscle. 00:30 In newborn disease, this is often because the mother has Myasthenia Gravis. 00:35 So mothers with Myasthenia Gravis have transplacental migration of their immunoglobulin or IgG which is direct against Neuromuscular injuctions. 00:45 This crosses the placenta and then attacks the infants neuro muscular injuction. 00:50 Infants may be sick for several weeks before they resolve as immunoglobulins can persist for a long time in the child after transplacental migration from the mother. 01:02 Patients present with fatigable weakness and they may have ocular muscle problems. 01:08 This is common especially early in disease. So they have a disconjugate gaze. 01:13 They can also have Ptosis and they often have diplopia. 01:18 Diplopia is not going to be a complaint that a child is going to have. 01:22 But you will see the disconjugate gaze. 01:24 Older children, who are already developing Myasthenia Gravis because they are having their own autoimmune event, will complain of Diplopia. 01:31 Myasthenia Gravis is caused by antibodies directed against the acetyl-choline receptor. 01:38 And these antibodies can absolutely be measured. 01:41 So the diagnosis is made by simply checking for the auto antibodies. 01:45 However, false negatives can occur. 01:47 And in cases where we suspect Myasthenia Gravis, we can do nerve conduction studies to make that diagnosis more definitively. 01:55 Another definitive way to make the diagnosis is to do the Tensilon test. 02:00 Remember, tensilon is effective because in patients with Myasthenia Gravis, tensilon will prevent the reuptake of the acetyl-choline and will cause a transient increase of Acetyl-choline in the Neuromuscularinjunction. 02:17 As a result, the patient should have a transient loss of symptoms. 02:21 The provision of tensilon should make the patient essentially improve immediately. 02:26 Treatment of Myasthenia Gravis involves providing Acetyl-cholinesterase inhibitors. 02:32 such as pyridostigmine. 02:33 These prevent the breakdown of acetyl-choline breakdown in the neuromuscularjunction and improve neuromuscular signalling. 02:41 Additionally, patients can have immunosupression to prevent the auto antibodies. 02:46 Prednisone is our mainstay therapy. 02:49 IVIG and plasmaphoresis can also be used to prevent those immunoglobulin from attacking the neuromuscularjunction. 02:58 Thymectomy is not recommended in children the way it is in adults. 03:03 In adults that can be curative. 03:04 But in children the thymus is crtically important for the developing of T-cells. 03:09 The thymus is actively involved in developing those T-cells throughout childhood. 03:13 So, we will not due thymectomy on prepubertal children. 03:18 That is all I have to talk to you today about this problem. 03:21 New Entry 51
About the Lecture
The lecture Myasthenia Gravis in Children by Brian Alverson, MD is from the course Pediatric Neurology. It contains the following chapters:
- Myasthenia Gravis
- Management of Myasthenia Gravis
Included Quiz Questions
Which of the following is NOT recommended in children with myasthenia gravis?
- Thymectomy
- Prednisone
- Intravenous Immunoglobulin
- Plasmapheresis
- Acetylcholinesterase inhibitors
Which of the following statements about Myasthenia Gravis is TRUE?
- It is the autoimmune attack of antibodies against ACH receptors in the post-synaptic muscle.
- It is exclusively found in children below the age of 2 years.
- It is a fatal disease leading to respiratory failure.
- It is a chronic nerve instability resulting in fatigability.
- In newborns, it is due to transplacental migration of maternal IgM against the ACh presynaptic receptors.
A 2 week-old child is brought with drooping of the eyelids at 2nd day of life. The mother also mentions the child "gets tired quickly". On physical examination, you notice ptosis of the eyelids while the child is feeding. What is the probable diagnosis?
- Transient myasthenia gravis
- DMD
- Becker’s muscle dystrophy
- Botulism
- Hypothyroidism
Which of the following does not contribute to the diagnosis of Myasthenia Gravis?
- Dexamethasone suppression test
- Tensilon test
- EMG
- Anti-cholinesterase test and muscle biopsy
- Antibody test
Which group of muscles are often affected first in Myasthenia Gravis in children?
- Ocular muscles
- Proximal muscles
- Distal muscles
- Muscles of mastication
- Intercostal muscles
Author of lecture Myasthenia Gravis in Children

Brian Alverson, MD
Customer reviews
4,0 of 5 stars
| 5 Stars |
|
0 |
| 4 Stars |
|
1 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Good lecture, it's important that it is part of the curriculum as I thought it was an adult disease. Thanks!
