Playlist
Show Playlist
Hide Playlist
Metabolic Acidosis – Laboratory Diagnostics

-
Slides DiagnosticsAcidosisAlkidosisStep1-2 RespiratoryPathology.pdf
-
Reference List Pathology.pdf
-
Download Lecture Overview
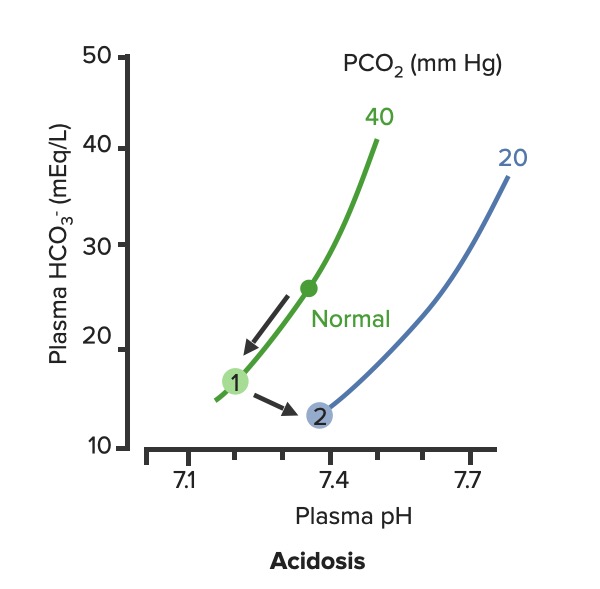
00:00 Let's continue. 00:02 Well, where we are here with the metabolic acidosis, after calculating our anion gap, will be – whether it's anion gap or non-anon gap. What does that even mean? Well, you calculate your anion gap and you find your sodium minus your anions. 00:20 What are they again? Bicarbonchloride. 00:22 And say that you find your anion gap to be above 12 and say that it's 25, there is a very interesting mnemonic that comes into play and comes in quite handy, it's called MUDPILES. 00:32 And this will be methanol, formic acid. 00:34 You're worried about if it's untreated, worried about blindness. Do not forget that. 00:38 Formic acid a metabolite of your methanol responsible for blindness if untreated. Uremia. 00:44 What does that mean to you? A renal failure. 00:47 You're going to be accumulating acid – metabolic acidosis, DKA; diabetic ketoacidosis. 00:54 You are increasing the production of ketones like crazy. β-Hydroxybutyric acid, acetone, ascetic acid. 01:02 P, we have propytene glycol. Iron tablets or INH for I. Lactic acidosis. 01:11 Ethylene glycol which is a component that may be found with antifreeze. And then salicylates. 01:18 So now be careful. So salicylates, when did you last see salicylate? In the previous discussion, you saw salicylates. 01:27 Let me bring this to your attention. Under respiratory alkalosis which means that early on with salicylate, it stimulates the respiratory center and then ended up what? With respiratory alkalosis. 01:39 What category am I in here? This is metabolic acidosis. At some point what is salicylate? It's an acid that you're ingesting. 01:48 So you end up having within this metabolic acidosis anion gap type. 01:52 The non-anion gap metabolic acidosis, we'll call that normal would be, well, you take a look at the mnemonic. 02:00 I'm gonna refrain from saying it. H- hyperalimentation. 02:05 A- Addison's disease. R- renal tubular acidosis. Which ones do you wanna know? One, two, four. Which one is a severe normal anion gap metabolic acidosis of the three? Type I, type I, type I. 02:23 Take a look at Addison's. What's that mean? Oh no, I don't have enough aldosterone. 02:27 So therefore I'm holding onto my hydrogen. Welcome to normal anion gap, metabolic acidosis. 02:34 Acetezolamide can actually be a part of what? What do you mean could be part of what? Acetazolamide does what? And if it's carbonic anhydrase, where are you? In your nephron. 02:44 In the proximal convoluted tubule. 02:46 If you knock out that carbon – carbonic anhydrase in the proximal convoluted tubule, you are unable to reabsorb bicarb. What kind of RTA or renal tubular acidosis would this be? Type I, type II or type IV? Remember that little clue that I gave you. 03:02 You need two lines to create an X so therefore this would be type II. 03:07 Spinorolactone and Addison's have something in common. What is that? The fact that aldosterone doesn't function properly. 03:14 Either in Addison's it's not being produced at all, in spironolactone you're blocking it. 03:18 This could – goes back. Once again, we discussed aldosterone in such great detail in nephrology. 03:24 We talked about how normally it does certain things such as reabsorption of sodium and gets rid of the hydrogen and potassium. 03:31 If you don't have aldosterone, then please understand that you have metabolic acidosis normal anion gap. 03:39 Saline infusion it also result in a normal anion gap type of metabolic acidosis. 03:45 These are important clinical differentiations. What are we referring to? Metabolic acidosis, you tell me about bicarb right now. Good. On the decreased side. 03:55 And what about your carbon dioxide? Most likely decreased as well. 03:59 Let me give you another point. When you find carbon dioxide and bicarb both moving in the same direction, and by that, I mean, here is my bicarb and it's a decrease giving you metabolic acidosis which your only method of compensation – hyperventilation – felt a little dizzy right there. 04:19 But blowing off carbon dioxide, it's also decreasing and that takes place within minutes. 04:24 If you get rid of your carbon dioxide, what are you trying to do? Compensate for the acidosis. 04:28 That should be clear. Understand every single term that I've mentioned there. 04:33 You may use these mnemonics if it helps you to come up with the two categories of anion gaps.
About the Lecture
The lecture Metabolic Acidosis – Laboratory Diagnostics by Carlo Raj, MD is from the course Pulmonary Diagnostics.
Included Quiz Questions
Which of the following is a metabolite of methanol that causes loss of vision?
- Formic acid
- Oxalic acid
- UDP
- 5-methyl folate
- Salicylate
The presence of oxalic acid crystals in a patient with anion gap metabolic acidosis points out towards which of the following etiologies?
- Ethylene glycol
- Propylene glycol
- Methanol
- Iron tablets
- Isoniazid
Which of the following causes the most severe form of non-anion gap metabolic acidosis?
- Type I renal tubular acidosis
- Type II renal tubular acidosis
- Type III renal tubular acidosis
- Type IV renal tubular acidosis
- Type V renal tubular acidosis
Which of the following causes a non-anion gap metabolic acidosis by altering the effect of aldosterone?
- Spironolactone
- Acetazolamide
- Saline infusion
- Iron tablets
- Ethylene glycol
Author of lecture Metabolic Acidosis – Laboratory Diagnostics

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Great explanation, details, logarithms and discussion. Great lecturer, thanks Dr Raj
