Playlist
Show Playlist
Hide Playlist
Meningeal Tumors: Meningioma

-
Slides 08 Tumors of the CNS Neuropathology II.pdf
-
Download Lecture Overview
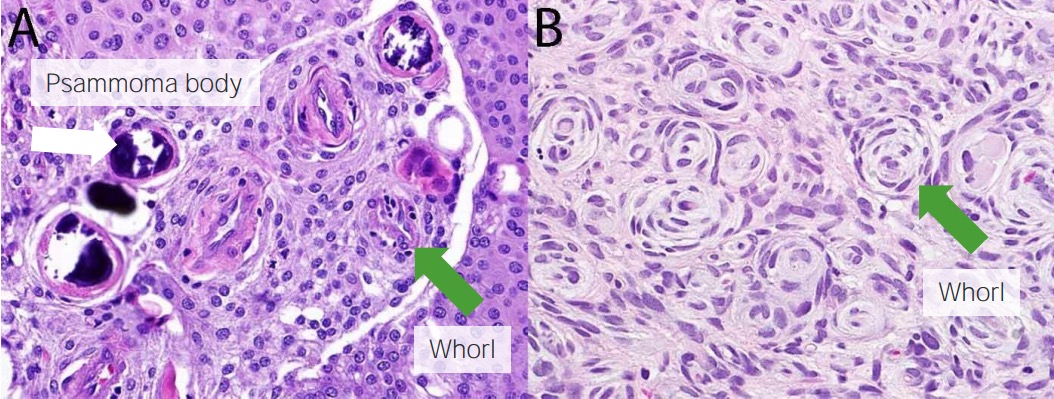
00:02 At this juncture, we’re moving onto a different classification. 00:06 A different classification of primary CNS tumors. 00:11 Up until now, we have completed officially our discussion of neuroepithelial tumors. 00:19 Under meningeal tumor, we’ll begin by looking at meningioma. 00:24 You want to keep your meninges separate from the brain parenchyma, please. 00:28 Anatomically, physiologically, pathologically for every reason possible. 00:33 So therefore, with that said, arises from the meningoepithelial cells or meningothelial cells of the arachnoid. 00:41 Think about where you are now. 00:43 Now, the growth, vast majority are benign. 00:48 Whenever you say the word benign, it all depends on the behavior of the benign tumor. 00:53 Now if someone says that basal cell carcinoma is benign, basal cell carcinoma, benign skin cancer, extremely common. 01:02 Benign, but my goodness if it’s locally aggressive, could you imagine if this tumor was on the nasal region? And then all of a sudden, it starts growing locally, it will completely disfigure the face. 01:16 My point is, just because something is benign, it doesn’t mean that you are able to ignore it or neglect it. 01:23 Because this is a benign tumor, and what’s going to happen? You have this tumor that’s growing, growing, growing in the meningeal region. 01:32 What’s adjacent to it? The freakin’ brain, come on. 01:36 So therefore, be careful. 01:38 You want to memorize chromosome 22. 01:41 Slow growing lesion and that’s the part that’s dangerous, huh? Because your patient has no clue that this is occurring. 01:49 Asymptomatic, which is really scary, really scary. 01:53 And by the time the patient is going to present to you with this slow growing, benign tumor, could you imagine as to how big this tumor would be by the time presentation is taking place? Slow growing lesion that presents either with vague, non-localized type of symptom. 02:14 Or, well, it depends on the growth and location, right? With focal findings, referable to the compression of the underlying brain. 02:21 You can imagine as to how big this tumor would be in which finally your patient is going to present. 02:28 Common sites would be the following: parasagittal aspect of the brain convexity, the dura over the lateral convexity, wing of the sphenoid, olfactory groove, sella turcica, or even the foramen magnum. 02:45 But really, think about all the meninges covering the entire brain, and as you do so, go from one part of the brain or one part of the meningeal region to the other and you’ve given yourself a nice little story of where you would find your meningioma. 03:00 Now, these meningiomas may express progesterone receptors. 03:04 And rapid growth, therefore may be taking place during pregnancy has been in fact reported. 03:09 So that’s an important point there that you want to keep in mind with meningioma and really a very unique feature. 03:16 I would call this a clinical pearl, huh? Pathology of meningiomas. 03:22 It’s a rounded mass, well-defined. 03:24 We know that because it’s benign already. 03:26 Anything that’s benign will be well-circumscribed and then eventually, during presentation, will cause compression. 03:32 Easily separable from the brain parenchyma because we’re dealing with a meningioma. 03:37 It is an encapsulated neoplasm. 03:40 And we have overlying what’s known as hyperostosis of the skull and what that’s basically referring to is the fact that above the meninges, the bone is going to react. 03:50 Underneath the meninges, you have compression-like symptoms, is that clear? Tumor spreads in the sheet-like fashion along the dura. 04:00 And now the lesion range from firm to fibrous, but this is what you want to pay attention to. 04:05 Finely gritty and that’s because of extreme calcification. 04:10 We then refer to this in meningioma and this calcification is called psammoma body. 04:17 From now on, whenever you hear the term psammoma body, you automatically, pathologically, equate this to calcification by reflex, Obviously, psammoma bodies could be found in a number of places. 04:31 Here, apart from meningioma, you could find this with a common malignant ovarian tumor and that is then referred to as being your serous cystadenocarcinoma. 04:41 And there are many places that you would find psammoma bodies. 04:44 Meningioma would be one of these. 04:46 What does it mean to you? Calcification. 04:49 In this picture, a psammoma body is being shown to you. 04:54 And within that psammoma body, you’ll notice that increased eosinophilic or hyperchromatic type of structure. 05:01 And that solid inside that body – that solid structure then represents the calcium. 05:09 This is meningioma. 05:11 Please be able to identify psammoma body and in a patient who is then presenting with new onset seizures and has taken years for this to occur, meningioma should be pretty high on your differential. 05:26 Treatment is only necessary in some cases, and is based on tumor size and location, as well as symptoms, and patient age. 05:33 About half of all cases can be actively watching, with only about 25% of those patients needing any intervention. 05:40 Treatment consists primarily of surgery with pre and post op corticosteroids, though radiotherapy may also be needed. Chemo is rarely used in these patients.
About the Lecture
The lecture Meningeal Tumors: Meningioma by Carlo Raj, MD is from the course Tumors of the CNS.
Included Quiz Questions
Which chromosome is affected in meningiomas?
- Chromosome 22
- Chromosome 21
- Chromosome 12
- Chromosome 23
- Chromosome 20
What receptor is often expressed in meningiomas?
- Progesterone receptors
- Gonadotropin receptors
- Testosterone receptors
- Cortisol receptors
- ACE receptors
From what type of tissue do meningiomas originate?
- Cells in the arachnoid mater
- Cells in the dura mater
- Cells in the pia mater
- Osteoclastic cells
- Osteoblastic cells
What is the composition of a psammoma body?
- Calcium deposits
- Fat deposits
- Chlorine deposits
- Chondral deposits
- Glycogen deposits
Author of lecture Meningeal Tumors: Meningioma

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
