Playlist
Show Playlist
Hide Playlist
Management of Major Burns

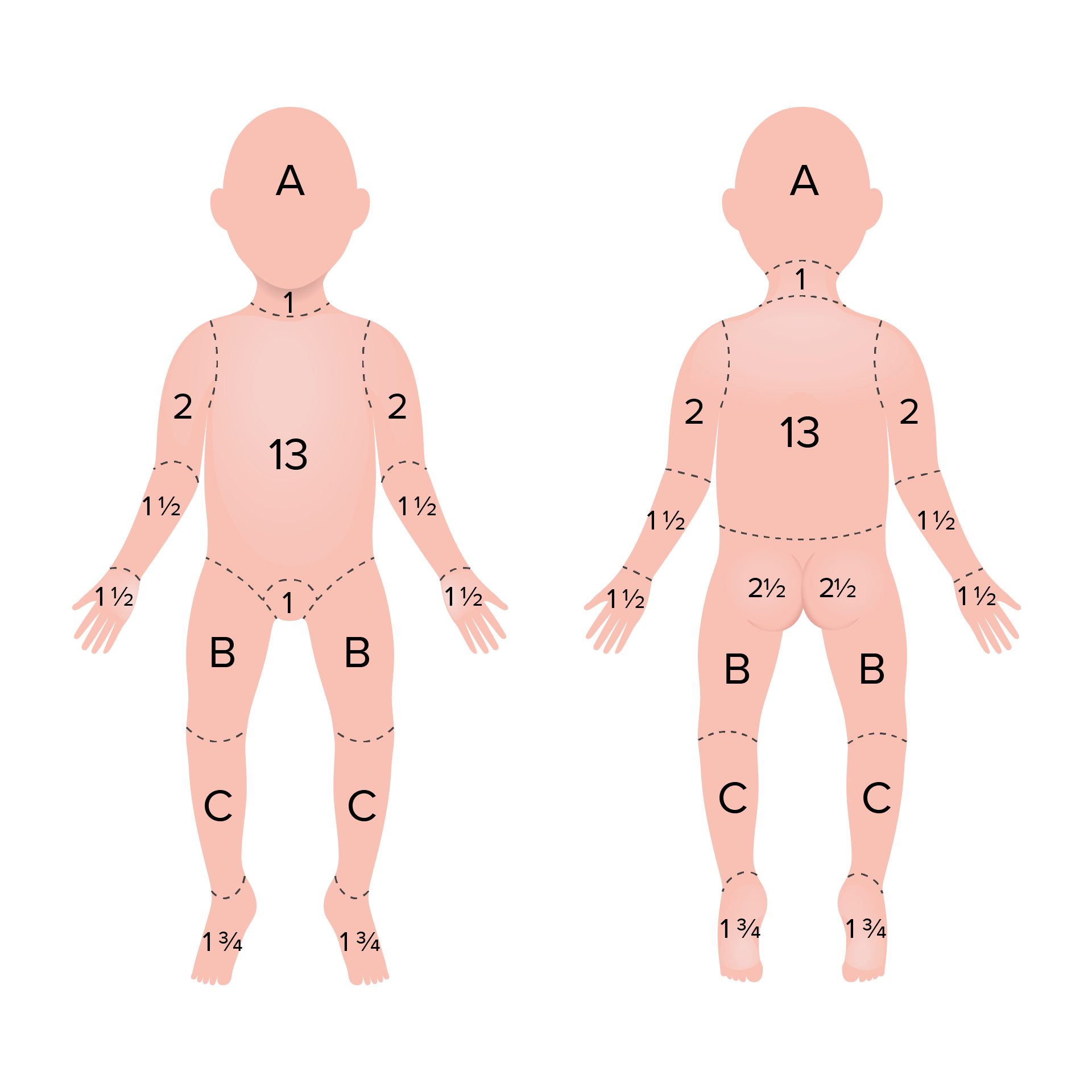
00:01 Management of burns if you get in the exam, it is no different to management of a normal trauma patient. 00:07 Exactly the same principles apart from couple of things you need to add. 00:11 In the breathing, and ventilation, you need to add carboxyhemoglobin and escharotomy. 00:18 What's the difference between escharotomy and fasciotomy? Yeah, you right. 00:26 So what is the difference in the incisions, for example? So what if you have a burn to the bone? Burn yeah, so the depth is does not create difference between the two In fasciotomy, you are going from the skin all the way up to the fascia, at least in the fascia, In the burn, it depends on the depth of the burn. 01:03 Usually, you do for a full thickness burn and you incise to fresh bleeding tissue. 01:11 So that might be in the deep dermis, it might be the hypodermis, it might be in the deep fascia, muscle or even the bone. 01:19 So their depth is depending on the depth of the burn. 01:23 The anatomical difference is, for escharotomy, you make your incisions along the axial lines, pre axial and post axial lines for escharotomy. 01:33 For fasciotomy is a different line. 01:35 So just for lower limb fasciotomy, you make two incisions here, 2 cm in behind the medial malleolus or behind the TBI here and 2 cm behind anterior border of the tibia. 01:47 So those are for you fasciotomy. 01:49 Okay, so escharotomy is pretty much only for burns. 01:54 And deep burns. 01:56 Okay. 01:58 So A, B, C, D, E, fluid resuscitation, specialist help, investigations, then these standard things. 02:22 Anything you want to ask in this? I'll come to the rule of nine's in the next couple of slides. 02:44 Yeah. 02:47 Okay. 02:50 Do you have a scenario or a question on what dressing you apply? Always go for cling film before we transfer the patient. 02:56 For the exam, make sure that don't mention (inaudible) or any of those the exam Go for cling film, that's what they expect you to answer. 03:08 Okay size of burns. 03:09 It affects the treatment and predicts mortality. 03:13 This is what he said, JP, palm of the hand is 1% including the fingers of the patient. 03:20 Okay, that's 1%. 03:22 Rule of nines is that 1%, so 9 times in the hand, in the leg is 18 times. 03:32 So this is all you need to remember. 03:35 Just as a rough percentage. 03:37 They will never ask you to estimate the accurate depth, the total body surface for the exam. 03:45 They'll just expected no rough approximately whether you are able to calculate it. 03:49 So just remember the rule of nines. 03:52 Rule of nines will apply to an adult or to a child more than 12 years old. 04:00 If they are less than 12, the body proportion is different. 04:04 For example in an adult the head is nine percent, but in the child is up to 18%. 04:11 In an adult, the leg is for 18%. 04:14 But in a child, it's much smaller 14%. 04:17 Okay? All you need to remember for the exam is this applies only for adults and more on 12 years old. 04:25 For less than 12, is a different formula, which is called the Lund and Browder chart. 04:32 Okay? Lund and Browder chart is a standard method in assessing burns. 04:38 In the burns, we use the Lund and Browder chart, because this is much more accurate than rule than rule of nines. 04:48 For the purpose of re-exam, in any department rule of nines, burns you need Lund and Browder. 04:56 Okay, you don't have to know why it is, but it is much more accurate in estimating the burn. 05:02 Depth above the burns affects of treatment, predicts healing time and scarring. 05:08 Now, be careful of this. 05:11 This is only depth they will give you on the exam, this is what you need to know. 05:15 Never get confused by reading any American books about first-degree, second-degree, third degree. 05:19 They will never ask you I never mentioned it. 05:21 It's always partial thickness, full thickness or superficial. 05:26 So in the skin, the epidermis is 5% of the skin thickness and the dermis is 95%. 05:35 So that part is superficial. 05:39 That's epidermal burned or superficial. 05:42 Then this part is called the papillary dermis. 05:44 This part is called a reticular dermis. 05:47 So that papillary dermis is superficial dermal or also called superficial partial thickness. 05:56 This is reticular dermis, deep dermal or deep partial thickness or anything beyond that is full thickness. 06:06 Okay, why is it important to know? Because for giving any scenario on burns what they will ask you is, what burn is this? Superficial. 06:16 It might be either a sunburn, it's not even a superficial burn. 06:20 It may be just a sunburn or going into the superficial burn or a epidermal burns. 06:24 So, this is probably the earliest burn. 06:27 This one? Partial thickness. 06:30 Why do you say partial thickness? Very good. 06:34 So superficial partial thickness not deep, because in deep partial thickness, you don't get the redness or unlikely to get blisters. 06:42 So if you have any scenario on redness, blisters, superficial partial thickness. 06:47 This says, more of superficial partial thickness areas here, but here is becoming more deeper. 06:56 A bit more deeper. 07:00 And well, pretty much deep dermal to full thickness. 07:03 You're right full thickness, you really see it scar. 07:06 Yeah, I agree with you. 07:07 This is more of deep to full thickness. 07:10 This is again deep dermal to full thickness. 07:13 Okay. 07:15 So in this, what is what? Epidermal, superficial, blisters, characteristic features, superficial dermal, white non-blanching skin, those characteristic spot for deep dermal and that is full thickness. 07:38 So in the exam, if they give you a burn with blisters, go for superficial dermal, also called superficial partial thickness. 07:54 Deep partial thickness. 07:56 Yeah, deep partial thickness because the full thickness they want to, the anatomy definition is hypodermis. 08:04 It has to involve the full layer of the epidermis, full layer of the dermis, then you go beyond that is full thickness. 08:12 So, hypodermis, fat, muscle, fascia, bone, are all full thickness.
About the Lecture
The lecture Management of Major Burns by Stuart Enoch, PhD is from the course Trauma and Post-OP Management.
Author of lecture Management of Major Burns

Stuart Enoch, PhD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
