Playlist
Show Playlist
Hide Playlist
Mallory Weiss Syndrome

-
Slides GD Esophagus.pdf
-
Download Lecture Overview
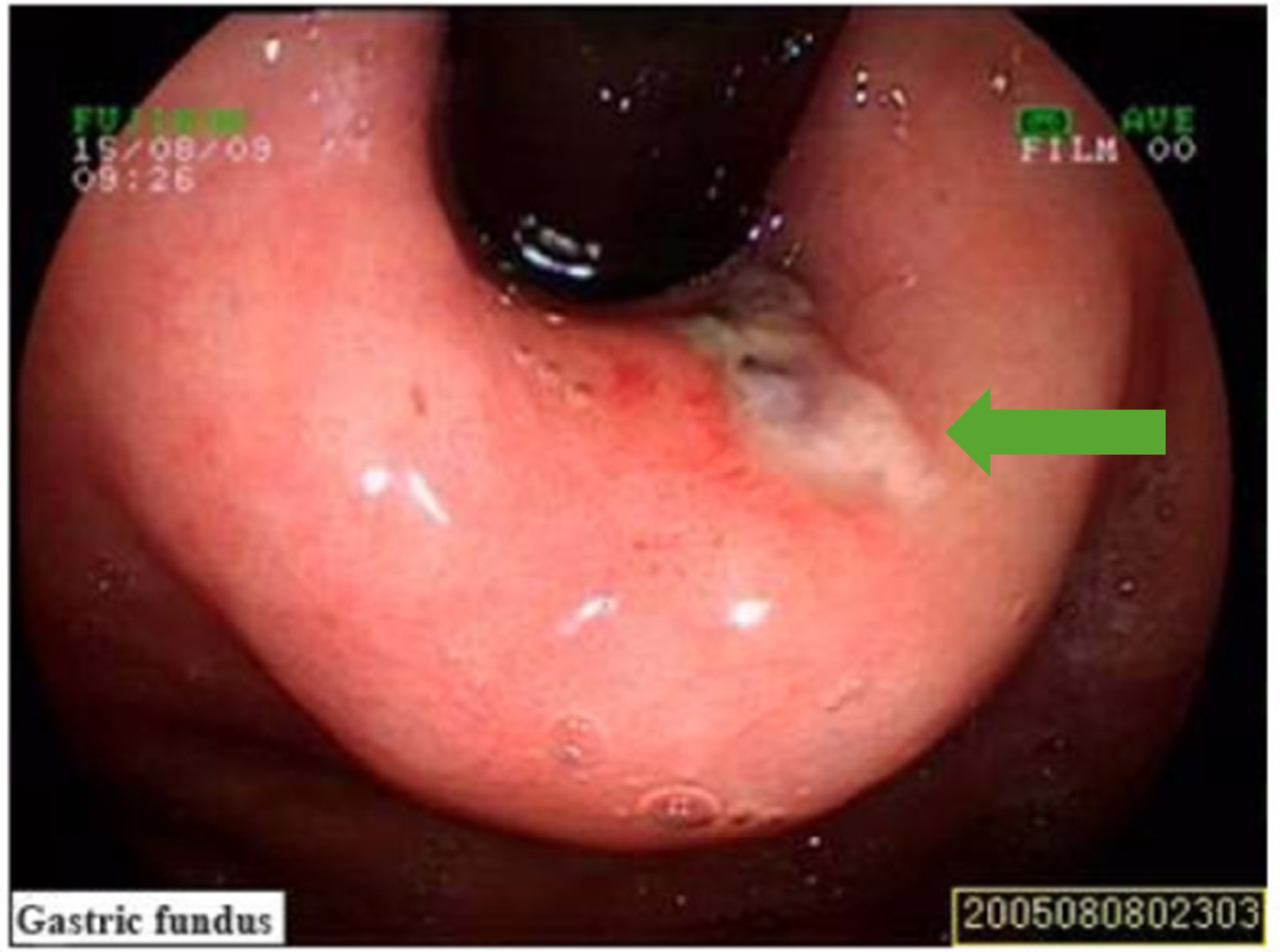
00:01 Our topic now, back in the esophagus is Mallory Weiss Syndrome. 00:08 Mallory Weiss Syndrome; what is your patient doing? Your patient could be the following: male or female, in the fashion industry, or high pressure image okay, image. 00:23 Maybe a poster child for Vogue. 00:27 You know one of these… or maybe a model for Victoria Secret or model for Calvin Klein would have you. Okay. 00:34 Your patient, might be a med student such as yourself. 00:40 Patient may be a law student, a highly stressful situation. 00:43 And every single weekend they find themselves binge drinking, binge drinking, binge drinking. 00:49 So I’ll give you two major populations here. 00:51 Binge drinkers where every weekend, every weekend they’ve taken high stress exams and such, you know what that is? But then they have to find relief, and outlets. 01:04 And so therefore, they binge drink every weekend and when they do so, [gags twice], right? They’re doing that quite a bit - retching. 01:12 I gave you the fashion industry, high pressure to maintain image of the body to the point where psychologically it becomes very, very draining. 01:24 So now they feel guilty about everything that they’re eating. 01:26 They had two fries, they run to the bathroom, [gags], you get the point. 01:32 So there’s quite a bit of increased pressure in the lumen of the esophagus. 01:38 Retching, or maybe vomiting. 01:41 When this occurs, then you’re worried about a tear taking place in your lower portion of your esophagus, posterolateral. 01:50 It’s the weakest portion. 01:52 This tear is then referred to as being your Mallory Weiss tear. 01:56 Mucosal laceration of the gastroesophageal junction, accounts for all 10% of your GI bleeds. 02:02 That’s pretty high isn’t it? The tear. 02:06 75% of the cases have history of recent retching, meaning increased interluminal pressure within the esophagus. 02:15 Repeated emesis, emesis, emesis. 02:18 Many of your patients actually have a hiatal hernia. 02:22 What does that mean again? The hiatus at T10 of the diaphragm becomes widened, you have herniation of the fundus perhaps sliding into the thoracic. Imagine a lot of bit of retching and emesis taking place. Spontaneous cessation, in 75% of your cases. Endoscopic cautery; so now what do you want to do? Literally you’re going to go in there and ‘sew the tear together’. But the ‘sewing’ will be taking place through cauterization. So endoscopy not only is going to give you… will help you diagnose, but then also here, helps you with management. Clipping, injection of epinephrine stops the bleeding. It’s important. 03:06 Mallory Weiss, you might be looking at vomiting but then it would be your hematemesis, vomiting up of blood because of a tear. 03:16 Keep in mind, this is a tear and not a rupture. 03:20 This is a tear, not a rupture. 03:23 Why do I keep repeating that? Two different diagnoses. 03:27 And the prognosis changes completely when you go from a tear to a… boring a hole through your esophagus. 03:36 Why’d I say it like that? Boerhaave Syndrome is boring a hole through your esophagus. 03:42 Your patient’s dead, high mortality. 03:45 Let’s go ahead and look at a tear here, on upper endoscopy. 03:49 On your left, where the arrow’s pointing to would be literally because of a recent history of a patient who had body dysmorphic syndrome, who then retched, retched, retched every time he ate something, resulting in a tear. 04:07 You’ll notice around it that there’s erythema because of the bleeding. 04:11 After endoscopic cauterization, you put the lesion back together. 04:17 In other words, you sewed it up.
About the Lecture
The lecture Mallory Weiss Syndrome by Carlo Raj, MD is from the course Esophageal Disease: Basic Principles with Carlo Raj.
Included Quiz Questions
A 19-year-old woman comes to the clinic complaining of severe vomiting of blood for 1 week. She has been on a strict diet, and her BMI is 16. You decide to do an endoscopy. Which layer of the esophagus would MOST likely be injured in this condition?
- Mucosa
- Submucosa
- Muscularis layer
- Serosa
- Lamina propria
A 35-year-old high-profile model presents to the emergency department after an episode of severe bloody vomiting, after which she passed out. On examination, her blood pressure is 100/40 mm Hg. You order a CBC to evaluate for anemia and then diagnose the condition as Mallory-Weiss syndrome. Which of the following is the BEST next step in management?
- Endoscopic cauterization to stop the bleeding in the esophagus
- Barium swallow
- Esophageal manometry
- Evaluation for GERD
- Prescribing anti-inflammatory drugs
Author of lecture Mallory Weiss Syndrome

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
