Playlist
Show Playlist
Hide Playlist
Macrocytic Anemia: Clinical Pathology

-
Slides Macrocytic Deficiency.pdf
-
Reference List Pathology.pdf
-
Download Lecture Overview
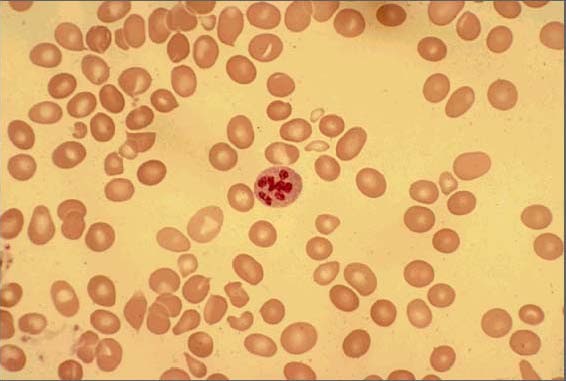
00:01 But macrocytic what are we looking for? Lab findings: decreased hemoglobin, increased MCV, more than 100. 00:10 Folate deficiency. 00:12 Now, pay attention here because we will not differentiate between folate and B12 deficiency. 00:16 If it's folate, you will have increased homocysteinemia or hyperhomocysteinemia. 00:23 B12 (deficiency) - decreased serum B 12. 00:26 And what was that enzyme that B12 was a cofactor there? MethylmalonicCoA or methylmalonyl mutase, right. 00:34 And then if it was homocysteine, you're dealing with methionine synthase. 00:38 Letter M stands for B12. 00:40 Signs and symptoms of anemia with macrocytic. 00:43 Now, under B12, I'm going to first walk you throughthose neurologic symptoms that I was referring to earlier when I was referring to our attaxic gait, spinal, cerebellar. 00:54 If it's proprioception and positive Romberg, that'd be posterior column or dorsal column. 00:58 And that corticospinal tract would then give you a positive Babinski sign referring to your premotor neuron lesion. 01:06 You're taking a tongue depressor, and in an adult, you take the lateral aspect the foot and you caress it as you do so. 01:13 As an adult, normally, we should then flex your toes, okay. 01:17 However, if it's positive Babinski, in an adult, where the toes then fan out upon lateral caressing of the toe, or excuse me lateral caressing of the foot. 01:26 Then this is going to be a sign of upper motor neuron lesion. 01:29 And this is not good, this is not good. 01:32 Last little thing that I wish to add in here and just stick with me, and physiology aspects of treatment of B12 deficiency. 01:41 And boards love asking questions like this, so that they know that you know that you have an understanding of B 12. 01:48 Earlier I said that if you find a substance within your urine, upon consumption of it, or that food or whatever it may be, then you know that it had to have been reabsorbed first, then filtered and gotten into urine. 02:04 Okay. Let me walk you through the following. 02:08 Your patient has all the signs and symptoms of B12 deficiency. 02:11 There is a megaloblastic anemia and unfortunately, there is neurologic deficit that's occurring. 02:16 And now the neurologic deficit is going to be irreversible. 02:20 Now, you don't find any B12 in the urine, because whatever that the patient is not consuming, let's say now, there's diet deficiency, either in a nursing home with an elderly patient, or maybe maybe it's a vegan that we talked about for years, years. 02:37 Well, now at this point, there's consumption of it, and there's supplementation of B 12. 02:42 And there's no problem inside your body. 02:44 It's just lack of diet, right. 02:47 So therefore, after consuming it, you can then expect to find B12 in your urine because then it has been reabsorbed and filtered and then taken up to liver and so forth. 02:58 Keep that in mind. 02:59 Now understand though, in a true Schillings test, you would then have to saturate all the receptors on the liver for B 12. 03:06 And that will not be asked because that's radiolabeled. 03:09 But the concept here becomes important. 03:12 Next, well if your patient had B12 deficiency, and now at this point, you're suspecting that is that is something like Pernicious anemia? Well, let's say that you give intrinsic factor. 03:27 And now you find that there's reabsorption of B12 from the terminal ileum into the plasma, and it's been filtered. 03:36 Well, let's say that you give intrinsic factor, and you still do not find the B 12 in the urine Your diagnosis cannot be Pernicious anemia. 03:45 So what's your next step? Need to find out where it is B12 deficiency occurring? The diet doesn't help with supplementation, intrinsic factor didn't help. 03:54 Let's go ahead and give this patient and pancreatic enzyme. 03:56 Would you tell me physiologically why you require a pancreatic enzyme? Good. 04:01 To remove the R factor from a B 12.S o that it then gets properly reabsorbed in the terminal ileum with intrinsic factor. 04:10 So now you give pancreatic enzyme and you find B 12 in the urine. 04:14 What's your diagnosis? Pancreatitis. Good. 04:17 So now, let's say the diet didn't work with supplementation, the intrinsic factor didn't work. 04:22 How do you know? Because he ended up finding it the B12 in the stool, and it wasn't in the urine. 04:27 Andpancreatic enzyme you had given, that didn't work. 04:32 Next, maybe you give antibiotics, you give antibiotics and you find B12 in the urine. 04:37 Theoretically, what happens here? Well, your diagnosis should be? Good. Back to overgrowth, right. 04:42 So back to overgrowth there, you kill off the overgrowth with antibiotic. 04:47 The B12 is now properly reabsorbed and ends up in the urine. 04:51 Do you understand the concept of how there are certain attributes of the Schilling test that you're going to use from head to toe so that you can then properly diagnose the patient. 05:02 And how they will most likely work this with B12 is going to be the fact that yo have cobalamin, okay? C-O, Cobalamin, keep that in mind. 05:10 And whether or not you find that in the urine and that table that I showed you with B12 , all the different methods by which you can develop it is important. 05:19 aLst little thing that I wish to bring to your attention, Is it megaloblastic anemia that you only find? meaning megaloblastic RBCs. 05:27 No, remember that the neutrophils also are not properly developing because as pancytopenia, you would expect to find, what can you think of what a normal neutrophils should look like? Okay, should they be segmented? Yes. 05:41 But what if you end to end up finding 8 to 12 segments? That's called a hypersegmented neutrophil. 05:48 And that to you should clue you in. 05:50 Oh, I must be suffering from or the patient's suffering from megaloblastic anemia. 05:55 Last little bit that I wish to bring to your attention is earlier, when I set up the overview for anemias I said that there was megaloblastic and non-megaloblastic anemia. 06:05 Up until this point, your focus should be strictly upon megaloblastic anemia. 06:10 And where's my problem with megaloblastic anemia? It's effect in DNA, or in the bone marrow, you don't have proper maturation, maybe either due to lack of DNA synthesis, or as we saw with diamond Blackfan anemia, We have a problem with aerythroid progenitor, right? If it's non megaloblastic macrocytic, and then you're thinking about alcohol, liver disease or reticulocytosis, think about those: Liver has nothing to do with the bone marrow. 06:39 Alcoholism has nothing to do with the bone marrow. 06:41 and reticulocytosis means a bone marrow is producing too many reticulocyte which is immature RBC into circulation. 06:51 Would you tell me the size of a cell that is always a little bit immature or premature than the mature cell The size, the size is always bigger. 06:59 So reticulocyte is always larger than an RBC. 07:03 And so therefore, you can have non megaloblastic macrocytic anemia, The big ones here, liver disease, alcoholism, and reticulocytosis. 07:15 Keep those in mind and that gives you big time high yield information for all macrocytic anemias that you have to be familiar with on your boards.
About the Lecture
The lecture Macrocytic Anemia: Clinical Pathology by Carlo Raj, MD is from the course Macrocytic Anemia – Red Blood Cell Pathology (RBC).
Included Quiz Questions
Which of the following favors B12 deficiency over folate deficiency?
- Elevated methylmalonic acid
- Normal methylmalonic acid and homocysteine
- Elevated homocysteine
- Low methylmalonic acid
- Low homocysteine
Which parts of the spinal cord are mainly involved in severe vitamin B12 deficiency?
- Dorsal columns and lateral corticospinal tracts
- Ventral horn and dorsal roots
- Central gray matter and ventral columns
- Anterior and lateral columns
- Dorsal columns and ventral horn
Which of the following findings on the peripheral blood smear is pathognomonic for megaloblastic anemia?
- Hypersegmented neutrophils
- Blasts
- Nucleated erythrocytes
- Howell-Jolly bodies
- Rouleaux formation
Author of lecture Macrocytic Anemia: Clinical Pathology

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
2 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
No words to describe how good are all the lectures performed by Carlo Raj. High yield, entertaining, interactive, concise.
Concise and laser focus on the high yield facts. Lectures are interspersed with witty humor which does not stray from the subject matter. Refreshing.
