Playlist
Show Playlist
Hide Playlist
Lymphoma in Children

-
Slides Lymphoma Alverson.pdf
-
Download Lecture Overview
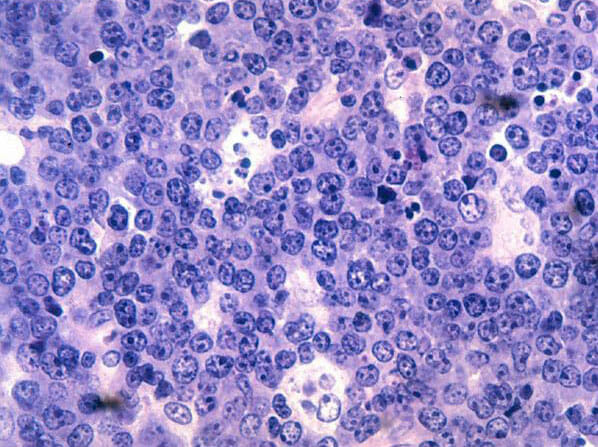
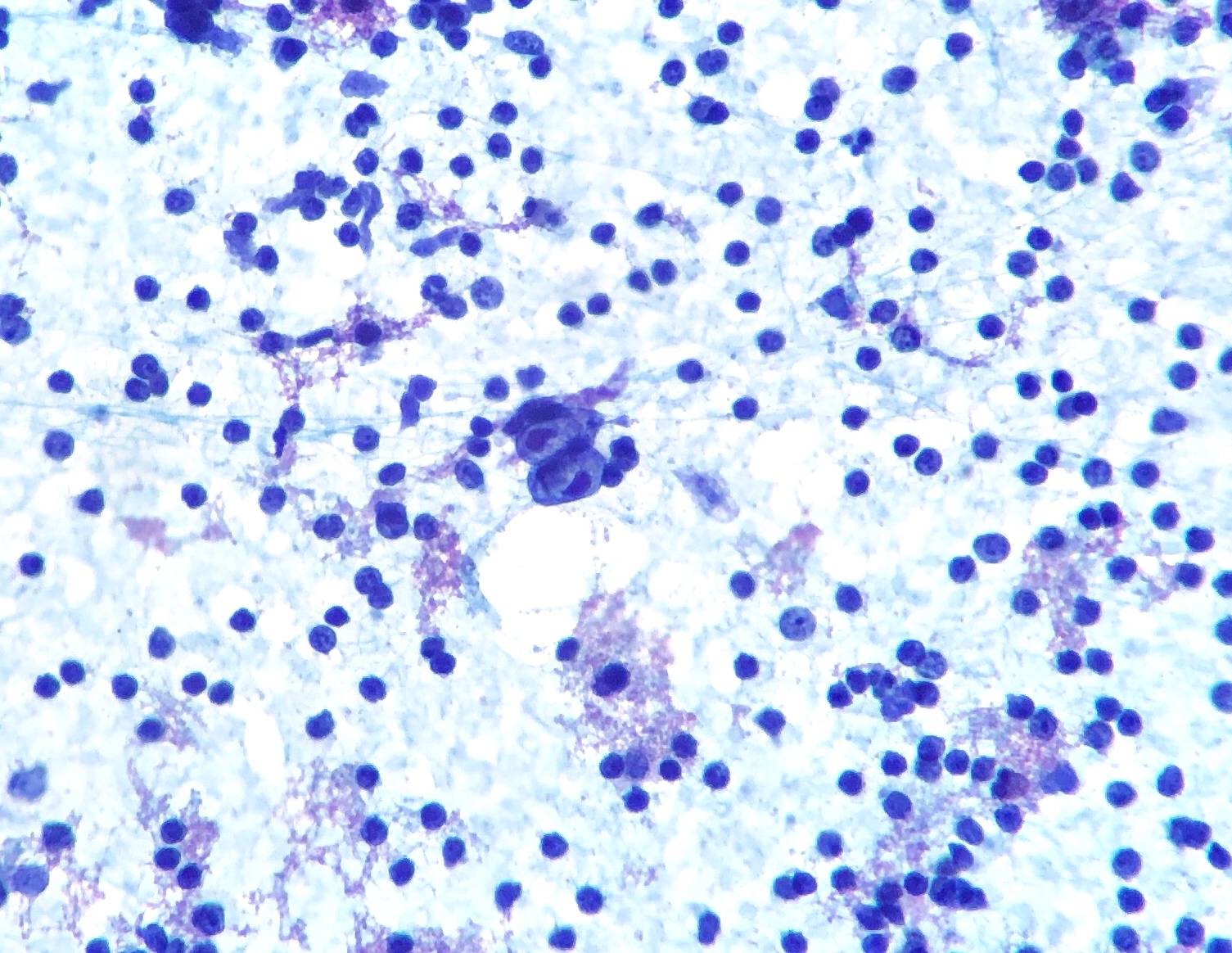
00:01 In this lecture we're going to cover lymphoma in children. 00:04 So let's review very briefly the origin of lymphoid neoplasms. 00:12 Basically you have T-cell and B-cell populations that can both create a variety of lymphomas as you can sort of see here demonstrated in this slide. 00:22 Not worth knowing all the details but do remember that they can stem from both lines. 00:27 So, there are 3 big time periods when people are at increased risk for lymphoma. 00:33 One is in childhood generally under ten years of age, another is young adults and adolescents generally ages 10 to 35, and then also later in adulthood after the age of 55. 00:46 We're going to focus on the kids. 00:48 So, there are several different types of lymphoma. 00:52 As I showed on the very first slide, this is probably one of the more famous ones, which is Hodgkin's lymphoma. This is a B-cell neoplasm. 01:00 So basically the B-cells become clonal and this happens typically in the germinal center of lymph nodes. 01:08 What you can see under a biopsy is this very classic finding of a binucleated cell we call the Reed-Sternberg cell. 01:17 It's supposed to look a little bit like an owl with big eyes. 01:20 So that multinucleated giant cell is malignant and these are embedded in the matrix of reactive cells and this is associated with EBV infections. 01:32 So, remember that connection of the Reed-Sternberg cell and the association with EBV for Hodgkin's lymphoma. 01:38 Generally, Hodgkin's lymphoma and many lymphomas will present with painless, matted, immobile lymphadenopathy. 01:48 You often see clumps of lymph nodes. 01:51 They are firm. They are rubbery, and they are immobile, and they do not hurt to palpation. 01:57 When you see this, this is lymphoma until proven otherwise. 02:01 So, what are some other key symptoms? Patients may develop an unexplained fever, they may have drenching night sweats, and they may experience weight loss associated with this malignancy. 02:15 So, if we suspect lymphoma, there's gonna be a few things we're gonna do. 02:20 First, we're gonna get some basic blood tests. 02:24 We're gonna get a CBC which may be abnormal or normal, and we're also gonna note markers of inflammation such as the erythrocyte sedimentation rate. 02:34 We can use the ESR to track efficacy of therapy. 02:38 So it's a good value to track chronically. 02:42 So, this will assess our response to therapy. 02:45 We're also going to do a biopsy on these patients to make a definitive diagnosis, often a bone marrow biopsy. 02:53 We can also biopsy an available lymph node and that's gonna evaluate the bone marrow involvement in which it's an important part of staging the disease. 03:03 We will also get scans of the thorax, and the abdomen, and the pelvis, and we'll do scans to look for other sites of activity because we wannna know whether this disease is localized to just those lymph nodes or spread throughout the body. 03:18 We can also do PET scans or bone scans as a way of assessing for how disseminated the disease has become. 03:26 So, that will allow us to stage the disease which is important because that will drive how we care for it. 03:32 So, let's go through the staging of of a Hodgkin lymphoma. 03:36 In Hodgkin's lymphoma, stage I disease is a focal area of just lymph nodes. 03:43 That's often in the anterior cervical chain. 03:46 Stage II is when the disease is mostly above the diaphragm or on one side of the diaphragm, as you can see on our person here. 03:56 He has some lymph nodes and also some mediastinal involvement and maybe 1 or 2 axillary nodes. 04:02 They're all on that side of the diaphragm. 04:04 Stage III is on both sides of the diaphragm and you may notice some splenic involvement as well, and stage IV is now when it's involving bone and liver and it is disseminated disease. 04:16 Okay, how we're gonna treat it is based on the stage and it's very complicated and these patients are basically plugged into a roadmap where they are getting certain stages of chemotherapy on certain days depending on how that disease is staged and age and a number of other factors. 04:35 But generally speaking, we're going to combine chemotherapy and radiation therapy to maximize our killing of these clonal cells. 04:43 Switching gears slightly to non-Hodgkin's lymphoma, these are malignancies that arise from lymphoidal cells and organs, and they're usually associated with immunodeficiency, and they may also be associated with viral infection like EBV which can cause Burkitt's lymphoma or HIV which can also cause a non-Hodgkin's lymphoma. 05:08 So, the key symptoms of non-Hodgkin's lymphoma are typically a rapidly progressive severity of illness in weeks to months. 05:18 These patients will often have hepatosplenomegaly, they will often have fever, and they may have some respiratory compromise from a rapidly expanding mediastinal mass. 05:29 They often can have abdominal obstructions and present with vomiting or inability to pass stool. 05:34 Testing for non-Hodgkin's lymphoma involves both blood tests just like in Hodgkin's. 05:41 You'll get a CBC and you will often see one of these cytopenias, either a neutropenia, or a lymphopenia, or anemia, or thrombocytopenia, and we often will get chemistry panels to assess for signs of tumor lysis syndrome which is when the cells are turning over very rapidly. 05:58 Examples of tumor lysis labs will be a high potassium, a high phosphate, or they may develop high uric acid or high LDH. 06:07 It actually isn't common for them to have tumor lysis syndrome prior to initiation of therapy but after initiation of therapy, this can be a real problem. 06:18 Additionally, we will scan these patients again to get a sense of how disseminated the disease is. 06:26 We will usually do chest x-rays and will often do a CT of the neck, chest, abdomen, and pelvis to look for lesions and then we also will do a bone biopsy to see if there is bone marrow involvement and we'll do a bone marrow aspiration and a lumbar puncture as well to assess of CNS involvement. 06:42 Again, like the other kinds of lymphoma this is a multi-agent systemic chemotherapy and it's based on the type of lymphoma it is, but in general, these patients have an outstanding prognosis. 06:57 Generally, patients with lymphoma do very well compared to adults with this similar disease. 07:04 So that's my brief review of lymphomas in children. 07:09 Thanks for your time.
About the Lecture
The lecture Lymphoma in Children by Brian Alverson, MD is from the course Pediatric Oncology. It contains the following chapters:
- Lymphoma in Children
- Hodgkin Lymphoma Staging
- Non-Hodgkin Lymphoma
Included Quiz Questions
A patient has been diagnosed with Hodgkin lymphoma with involvement of one lymph node region in the neck without any other findings. What stage lymphoma does this patient have?
- Stage 1
- Stage 2
- Stage 3
- Stage 4
- Stage 5
A cervical lymph node biopsy from a 10-year-old girl reveals a large cell with a bilobed nucleus with prominent eosinophilic inclusion-like nucleoli resembling an owl's eye. Which of the following is the most likely diagnosis?
- Hodgkin lymphoma
- Acute lymphoblastic leukemia
- Acute myeloid leukemia
- Non-Hodgkin lymphoma
- Tuberculosis
Which of the following types of lymphomas is most strongly associated with Epstein-Barr virus infection?
- Burkitt lymphoma
- Diffuse large B-cell lymphoma
- Mucosa-associated lymphoid tissue (MALT) lymphoma
- Mantle cell lymphoma
A child has been diagnosed with Hodgkin lymphoma. She has involvement of the axillary lymph nodes and spleen without involvement of other organs. What is the stage of this lymphoma?
- Stage 3
- Stage 1
- Stage 2
- Stage 4
- Stage 5
Author of lecture Lymphoma in Children

Brian Alverson, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
A complex topic made simple: the hallmark of a great teacher. Thanks!
