Playlist
Show Playlist
Hide Playlist
Systemic Sclerosis: Limited vs. Diffuse

-
Rheumatology I 04 Non Arthritic Connective Tissue Diseases.pdf
-
Reference List Pathology.pdf
-
Download Lecture Overview
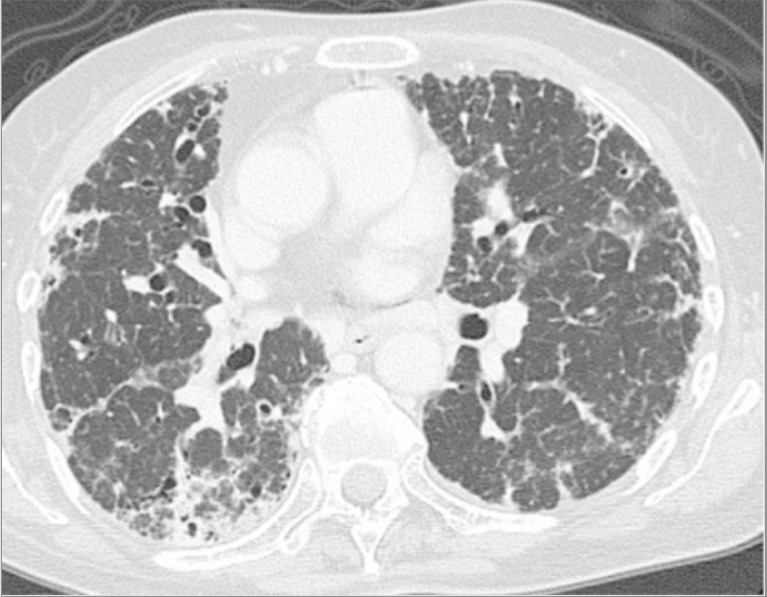
00:00 Our topic here is scleroderma. If it's one description that was to be given to scleroderma, it would be fibrosis. Let's take a look. Definition. It's exactly what it is, why it is fibrosis, but what if it was limited to the skin, then there'd be something called limited type of scleroderma and they'd be part of a constellation called CREST syndrome and if it was, remember CREST, C stood for calcinosis and you can also use that C for the marker for limited type of scleroderma which is anticentromere, the R would be for Raynaud, E esophageal dysmotility, S sclerodactyly, and T telangiectasia. So we're about to talk about scleroderma. 00:45 Let's begin. Sclero means scarring, derma of course we are referring to the skin; however, it doesn't always have to be limited to the skin, does it. So, if you have organ involvement or visceral type of sclerosis, then no doubt we have systemic. Unknown in terms of etiology, scleroderma usually affects middle-aged women autoimmune. Early lesions demonstrate vascular endothelial damage associated with autoantibodies and we'll talk about what those are in a second. Steroids will not be effective here because you have unlimited production of fibrosis. There are 2 types now, the systemic, the diffuse type. The diffuse type by definition not only would you have skin involvement but then also organs. The marker that we'll talk about with diffuse is called Scl-70. You may want to think about it as scleroderma 70. However, another name for Scl-70 is topoisomerase I. The limited type, what does that mean? You would have fibrosis taking place exclusively to the skin or only to the skin, maybe in the forearm. 01:56 Also has early development of pulmonary hypertension, there is a possibility, and you have small-vessel damage. So, the biggest difference, make sure that you know diffuse type which you have no doubt rampant and technical organ involvement, much more aggressive. That's the one that may kill your patient. If it's a limited type, skin, maybe the blood vessels. In the limited type, we have CREST. It's what C-R-E-S-T stands for. The symptoms are characterized by the following, let's talk about that CREST and let's first talk about Raynaud. Now Raynaud disease would mean if it's primary. The Raynaud disease will be primary which means that there was no underlying issue, it's not secondary. It will just be idiopathic. If it's Raynaud phenomenon, then it would be part of limited. Look for calcinosis, esophageal dysmotility, "doc, I'm having a hard time eating, hmmm." Take a look at the fingers and I'll show you in a little bit and it looks like the fingers of that of a witch, tapered, sclerodactyly. Now what happens first is the fact that you take the hand and you place it into the cold. Upon exposure to the cold, the little blood vessels in your fingers will start undergoing vasospasms, hmm. So now if the blood vessels within your digits undergo vasospasms, you're decreasing the supply of oxygen to your digits, correct. What's the 1st color do you think it'll first become? That's important. It won't be cyanotic immediately, will it, no, but it'll begin the process of cyanosis in the fingers. 03:30 So the 1st color you're going to go from, take a look at your finger here now, it's pinkish, right. You should have capillary filling and such. You put it out in the cold, at first vasospasms might then cause it to be white. Continued exposure and vasospasm will then cause it to become blue which is your cyanosis. You bring the hand back into the warmth, you're returning blood supply to the fingers. Now, it goes from being blue to dusky, ah, to red. That's the spectrum of colors that you want to know for Raynaud, white, blue, red, the colors of the flag; however, the order is a little bit different, right. Raynaud phenomenon, vasospasms taking place in your digits upon exposure to the cold. Sclerodactyly in CREST, the S, it means that the finger is undergoing tapering, thickening that I'll show you in a little bit. It's called sclerodactyly. Decreased facial skin, wrinkles because of, once again, scleroderma. Esophageal dysmotility, back to your overgrowth malabsorption syndrome. That's a possibility as well with CREST. You must understand that with CREST the type of scleroderma that you call this is limited in which the marker for this is ____ . Here we have the diffuse type of scleroderma. 05:03 Hmmm, things become a lot worse here. Not only may you have involvement of the skin but then you have end-organ involvement. Hmmm, imagine if the lung became fibrosed and you have decreased compliance. It'd be a very hard cased lung. In other words, you'll just form interstitial lung disease in which the alveoli may then perish, eventually may lead in to pulmonary hypertension. Oh boy, if that happens you'll be worried about right-sided heart failure, hemodynamic instability, not a good situation for the patient to be in. It could cause death. It could be cardiomyopathy of what kind please, restrictive. You just fibrosed the heart for Pete's sake. Next, there might be a fibrosis of intestine. That definitely is going to cause malabsorption and what you're worried about is your kidney. Could you imagine if fibrosis is taking place down in the renal? You lost your GFR, hypertension, may then go into RPGN within 3 months, 12 weeks, those kidneys are gone. Not good. You take a look at the fingers here, limited, and with limited, we have the arrows that are pointing to the areas that are fibrosed, tapered, thickening taking place. This is known as sclerodactyly. The type of inflammation that I showed you earlier on the hands, let's say of rheumatoid arthritis or even psoriatic arthritis, that was called dactylitis. That was inflammation. This is smooth, tapered fingers of the hand. Let's take a look at that nail fold even closer. So imagine now that the top portion of the 1st picture on the left represented the nail then down here is the cuticle and then within your cuticle obviously will then be your capillaries. The 1st picture on your left is normal. 07:03 Now, with sclerodactyly, you'll notice now that there's capillary dilation taking place in the middle picture and then there's something called capillary dropout. It is a part of the changes that are taking place with sclerodactyly. Diagnosis is scleroderma. Characteristic examination, look for the skin changes that we talked about where there's taut skin because of fibrosis. 07:29 ANA is usually positive but keep in mind that obviously it's not specific. Anti-Scl-70 is going to be specific for what type of scleroderma, diffuse. Another name for Scl-70 is anti-topoisomerase I. 07:47 If you find the marker being anticentromere antibody then this will be the limited type of scleroderma which will then be present in CREST. Management, really no effective treatment unfortunately available. Calcium channel blockers, we'll then be thinking of being used with Raynaud if the patient is suffering from limited type of scleroderma and Raynaud. Esophageal reflux, with the reflux, then you're thinking about perhaps using PPI, and if you're worried about renal issues, then you should be thinking about ACE inhibitors. Steroids and cyclophosphamide for interstitial lung disease, you're thinking about your modulators. The skin stretching exercises because things are becoming, even though the patient may look young it's pathological, so you need to make sure that you maintain proper mobility, and endothelin receptor antagonist, bosentan. Remember endothelin is an endogenous component that is being formed by the endothelial cell responsible and an extremely potent vasoconstrictor. 08:57 An endothelin-receptor I blocker such as bosentan could be used for the management of pulmonary artery hypertension that may take place maybe secondary to diffuse scleroderma.
About the Lecture
The lecture Systemic Sclerosis: Limited vs. Diffuse by Carlo Raj, MD is from the course Connective Tissue Diseases. It contains the following chapters:
- Introduction to Scleroderma
- Limited Scleroderma
- Diffuse Scleroderma
Included Quiz Questions
Which of the following diagnoses is most likely in a patient with dysphagia, calcinosis, Raynaud phenomenon, and positive anti-centromere antibodies?
- CREST syndrome
- Rheumatoid arthritis
- Mixed connective tissue disorder
- Systemic lupus erythematosus
- Diffuse systemic sclerosis
Which of the following is NOT a feature of limited systemic sclerosis?
- Inflammatory arthritis
- Esophageal dysmotility
- Sclerodactyly
- Raynaud phenomenon
- Calcinosis cutis
A 40-year-old woman presents with digital sclerodactyly and telangiectasias. Which of the following antibodies is most likely to be positive in this patient?
- Anti-centromere antibodies
- Anti-topoisomerase I/Anti-Scl-70
- Anti-cyclic citrullinated peptide
- Anti-double stranded DNA
- Anti-La/SSB antibodies
Which of the following is NOT recommended for the treatment of Raynaud phenomenon?
- Hydroxychloroquine
- Topical nitrates
- Amlodipine
- Warm gloves
- Nifedipine
Which of the following drugs is NOT recommended in the treatment of scleroderma?
- Adalimumab
- Amlodipine
- Omeprazole
- Methotrexate
- Cyclophosphamide
Author of lecture Systemic Sclerosis: Limited vs. Diffuse

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
