Playlist
Show Playlist
Hide Playlist
Less Common Lung Tumors

-
Slides 07 LungCancer Tumors and Metastases Neoplasias RespiratoryAdvanced.pdf
-
Download Lecture Overview
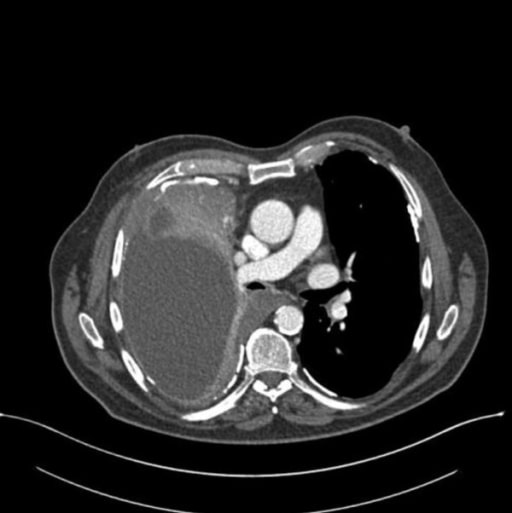
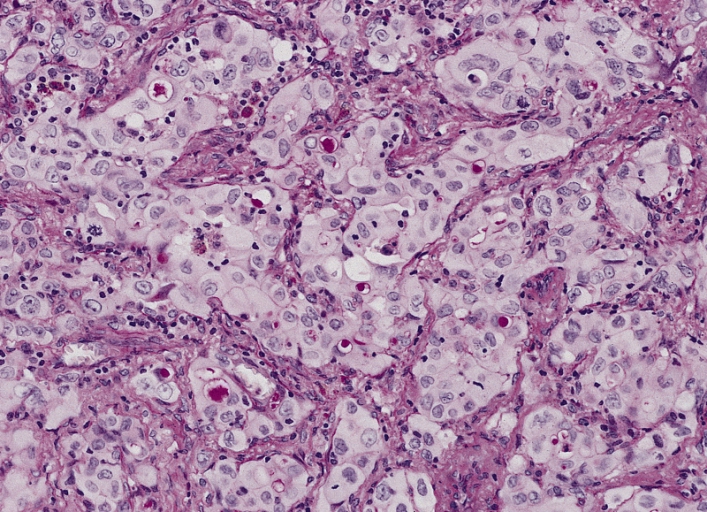
00:01 Less common tumors. Right, so there are several different types of tumours that can present with lung mass which isn’t a lung cancer. There are numerous different types, I have discussed three different types here today. They are often asymptomatic, nodules on a chest x-ray or they cause a bronchial obstruction with cough, haemoptysis or lobar collapse. They are not related to smoking and the patients tend to be younger than those who normally get lung cancer. 00:30 So probably the commonest ones are the carcinoid tumours. These are semi-malignant that means that they are not fully benign. They can spread and invade. They don’t tend to metastasize too much. But they are quite hard to treat because they do comeback after resection. They originate from neurosecretory cells of the bronchial mucosa. They tend to be central causing bronchial obstruction problems. Hamartomas are peripheral benign tumours that show up on chest x-ray, this is a CT scan of one. They have a distinctive CT appearance which is a little bit difficult to show on the scan but essentially they have variable tissues and types and that means they have variable density of the nodule on the CT scan. 01:15 Another semi-benign, semi-malignant tumour is adenoid cystic carcinomas which are of the large airways and again those are treated by surgical resection. 01:26 Metastases to the lung. We have discussed lung cancers. We have discussed mesothelioma which are definitely the predominant primary lung cancers. However the lungs are the site of metastases from many other tumours very frequently. So about 50% of patients with any type of malignant tumour will have lung involvement usually towards the end stage of the disease. It will represent stage 4 disease i.e. incurable disease. For most situations, there are exceptions. Testicular cancers for example and lymphomas can be treated even they were metastasize to the lung. Lung metastases present with four main patterns. 02:14 The x-ray can show masses and these might be single but usually a multiple, different sizes both of the lungs and that’s probably the commonest presentation. 02:28 Pleural effusions are also very common and they have present exactly how you might expect and the same is a pleural effusion due to lung cancer with metastases visible on the pleural, an odd sound on the CT scan that leads to the increasing size of an effusion over weeks and makes the patient breathless. And then you can get mediastinal node involved just like you do of lung cancer but with cancers elsewhere in the body, breast cancer, and prostate cancer for example. The fourth category is very unusual which is where you get the lymph vessels being filled up by the metastatic cancer. This is called lymphangitic carcinomatosis and this presents like an infiltration of lung disease with reticular shadowing on the x-ray and increasing breathlessness over time. 03:18 The important thing about lung metastases is that they represent stage 4 disease for the primary cancer. So if you have somebody with breast cancer and a lung metastases that’s stage 4 incurable breast cancer and the same for the gastrointestinal tract tumors. 03:33 So the lung involvement is key for the treatment of the primary cancer and that may require a biopsy to confirm that is the metastases. Because the implications of treatments for primary cancer are very important. So the common cause of lung metastases is lung cancer itself often metastasizes to other parts of the lung, same lung and to the different lung, head and neck cancer, breast cancer, the gastrointestinal, colorectal cancers, melanoma, and kidney cancer. The right side shows the proportion of patients with these different types of cancer who may have lung metastases at presentation. So if a lung cancer for example, nearly a third of patients will have a lung metastases at presentation. Kidney cancer 20% of patients.
About the Lecture
The lecture Less Common Lung Tumors by Jeremy Brown, PhD, MRCP(UK), MBBS is from the course Lung Cancer.
Included Quiz Questions
Which of the following are possible patterns of presentation of metastases to the lung by other primary tumors?
- All the options are possible patterns of presentation of metastases to the lung by other primary tumors.
- Intrapulmonary masses
- Pleural effusions
- Enlarged mediastinal nodes
- Lymphangitis carcinomatosis
Which of the following cancers does NOT commonly metastasize to the lung?
- Basal cell carcinoma
- Head and neck cancer
- Breast cancer
- Colorectal cancer
- Melanoma
Author of lecture Less Common Lung Tumors

Jeremy Brown, PhD, MRCP(UK), MBBS
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
